-
Patient Presentation
- Adult patient with confirmed GERD history
- Chief complaint: sensitivity, disliking the appearance of teeth, and “short teeth”
- No pain but noticeable aesthetic decline over several years
- Patient unaware that reflux was the primary cause of tooth
- destruction
- Clinical Findings
Generalized erosive surface loss across all 6 upper anteriors
Classic GERD pattern: palatal and incisal edge involvement
Cupped-out lesions, loss of incisal translucency
Generalized yellow-amber discoloration from dentine exposure
Reduced clinical crown height bilaterally
No active caries but compromised enamel integrity throughout
- Diagnosis
Erosive Tooth Surface Loss (ETSL) secondary to chronic GERD
BEWE score: moderate-severe
Tooth structure loss predominantly enamel with dentine involvement
Risk of further progression without systemic GERD management
- Treatment Planning
Medical referral reinforced for GERD control before committing to definitive restorations
Decision made for direct composite as first-line approach
Rationale: additive, reversible, conservative — no preparation required
Silicone index not fabricated in this case; free-hand layering technique selected
Shade matched to remaining tooth structure to blend naturally
- Procedure Steps
Full rubber dam isolation placed for moisture control and field clarity
Selective etching of enamel margins
Universal adhesive applied and light cured
Dentine shade composite placed as base layer to restore lost volume
Enamel shade composite layered incisally for translucency
Incremental build-up repeated across all 6 units
Initial contouring done under rubber dam
Dam removed — occlusal check and articulating paper adjustment
Final finishing and polishing with discs and rubber points
- Challenges Encountered
Severely reduced enamel available for bonding — adhesion reliability compromised
Maintaining consistent incisal edge level across all 6 units freehand
Color matching to heavily discolored underlying dentine
Patient’s ongoing GERD means restoration longevity is inherently limited without systemic control
- Result
Satisfactory restoration of incisal edge definition and crown height
Improved aesthetics with natural-looking composite layering
Patient reported immediate reduction in sensitivity
Smooth emergence profile and acceptable proximal contacts restored
- Prognosis & Follow-Up
Short-to-medium term prognosis: good, conditional on GERD management
Patient counselled on: avoiding acidic foods, using a soft toothbrush, fluoride application
Custom occlusal splint recommended to protect restorations at night
6-month recall scheduled for monitoring wear and marginal integrity
Long-term plan: ceramic veneers or crowns if erosion progresses despite treatment
- Key Takeaway
Always identify and address the underlying cause before restoring
Direct composite is an excellent interim or definitive solution in GERD erosion cases
The patchwork approach preserves tooth structure and buys time while the medical condition is managed
Patient education about GERD’s oral impact is as important as the restoration itself
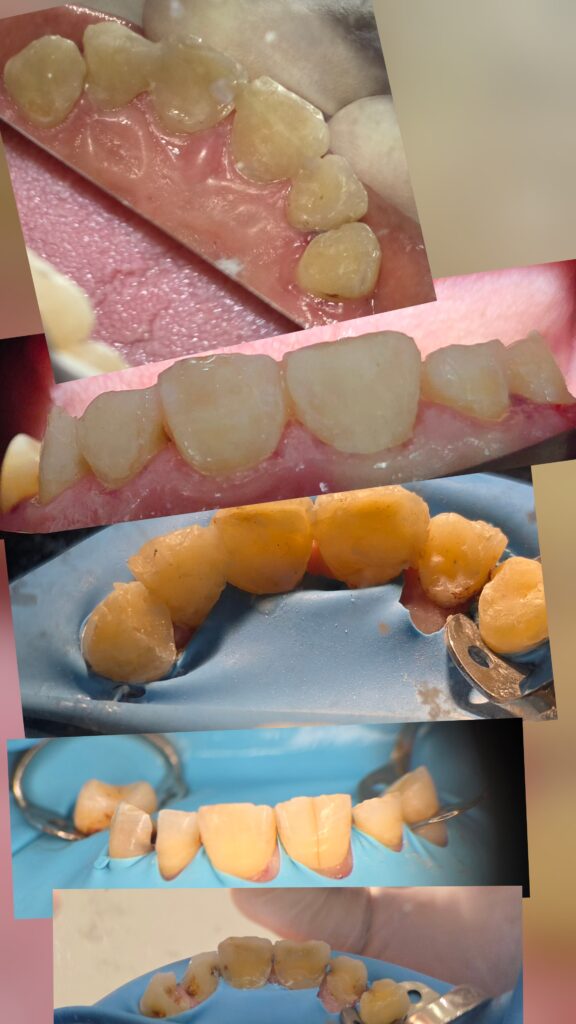
The entire case sequence

Post after finishing

Post before finishing and fixing the entire lingual surface

The condition labially pre

Condition pre xray

Another xray pre
Share on: