One of the most common causes of endodontic failure is the inability to identify and treat the complete root canal system. While clinicians are generally familiar with the typical anatomy of mandibular third molars and maxillary second premolars, anatomical variations continue to challenge even experienced practitioners.
The complexity of root canal morphology extends far beyond the number of roots or canals present. Canal merging, splitting, rejoining, and apical confluences can significantly complicate cleaning, shaping, and obturation procedures. Therefore, every case should be approached with the assumption that additional anatomical variations may exist until proven otherwise.
The following cases demonstrate uncommon three-canal configurations in a mandibular third molar and a maxillary second premolar, both presenting with intricate apical anatomy and canal convergence patterns.
Case 1: Mandibular Third Molar (Lower 8)
Diagnostic Assessment
Pre-operative radiographic examination revealed a mandibular third molar with an unusual canal pattern. Although third molars are among the most anatomically variable teeth in the dentition, identification of a true three-canal system remains relatively uncommon.
Careful evaluation of the radiograph suggested the presence of multiple canal spaces within the mesial aspect of the root. This finding prompted a conservative but thorough exploration of the pulpal floor.
Canal Anatomy
Following access cavity preparation and canal negotiation, three canals were identified:
- Mesiobuccal canal
- Mesiolingual canal
- Distal canal
The two mesial canals remained distinct throughout the coronal and middle thirds before converging into a single pathway in the apical third. The distal canal maintained an independent course toward the apex.
This configuration represents a complex confluent anatomy in which multiple canal systems eventually merge before exiting the root.
Clinical Considerations
Such anatomy presents several challenges:
- Difficulty in identifying all canal orifices.
- Increased risk of missing one of the mesial canals.
- Potential accumulation of debris within the canal isthmus.
- Increased complexity during irrigation and obturation.
Particular attention was given to irrigation activation and apical preparation to ensure adequate debridement of areas inaccessible to mechanical instrumentation.
Obturation was performed after confirmation of complete canal negotiation and working length control.
Case 2: Maxillary Second Premolar (Upper 5)
Diagnostic Assessment
Maxillary second premolars are traditionally expected to present with one or two canals. The presence of three canals is considered an uncommon anatomical variation and may easily be overlooked on conventional radiographs.
Initial assessment revealed radiographic signs suggestive of canal multiplicity. Careful exploration under magnification confirmed the presence of three distinct canals.
Canal Anatomy
Three independent canals were negotiated successfully:
- Buccal canal
- Palatal canal
- Additional accessory canal pathway
The canals remained separate through the majority of the root length. However, in the apical region, they demonstrated a complex convergence pattern, gradually joining into a common pathway before exhibiting a deep terminal division near the apex.
This morphology created an intricate apical architecture that would have been impossible to appreciate without careful radiographic interpretation and canal tracing.
Clinical Considerations
The greatest challenge in this case was understanding the relationship between the canals in the apical third.
Failure to recognize the apical confluence could potentially result in:
- Incomplete cleaning of the canal system.
- Transportation during instrumentation.
- Inadequate obturation of the entire anatomical space.
A cautious shaping strategy was employed to preserve the original anatomy while ensuring sufficient disinfection of the complex canal network.
Discussion
The root canal system should not be viewed as a simple collection of straight tubular structures. Instead, it represents a dynamic three-dimensional network capable of exhibiting considerable anatomical variation.
Both cases demonstrated a common feature: canal confluence.
In the mandibular third molar, two mesial canals merged before apical termination. In the maxillary second premolar, three canals followed separate trajectories before converging and subsequently exhibiting a deep terminal division.
These findings emphasize several important clinical principles:
- Radiographs should always be evaluated from multiple angulations.
- Canal anatomy should never be assumed based solely on tooth type.
- Magnification significantly improves the detection of additional canals.
- The clinician must remain alert for apical complexities even after all canal orifices have been identified.
- Successful treatment depends not only on locating canals but also on understanding their entire three-dimensional pathway.
Conclusion
These two cases illustrate the remarkable anatomical diversity that can be encountered in everyday endodontic practice.
A mandibular third molar presenting with three canals and mesial canal confluence, together with a maxillary second premolar exhibiting a rare three-canal system and complex apical convergence, serves as a reminder that root canal anatomy frequently defies expectations.
Careful diagnosis, meticulous exploration, and respect for anatomical complexity remain essential for predictable endodontic success.

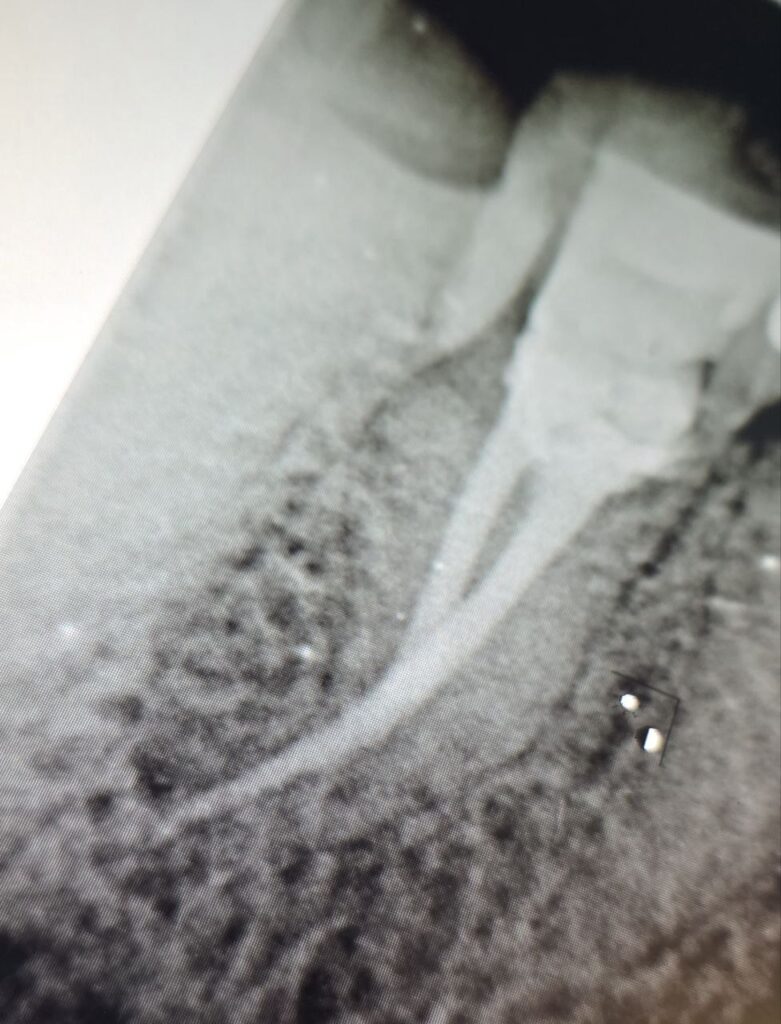
lower 8 with resin cement and lateral condensation obt
distal view of the 3d obt of the upper 5 with bioceramic sealer
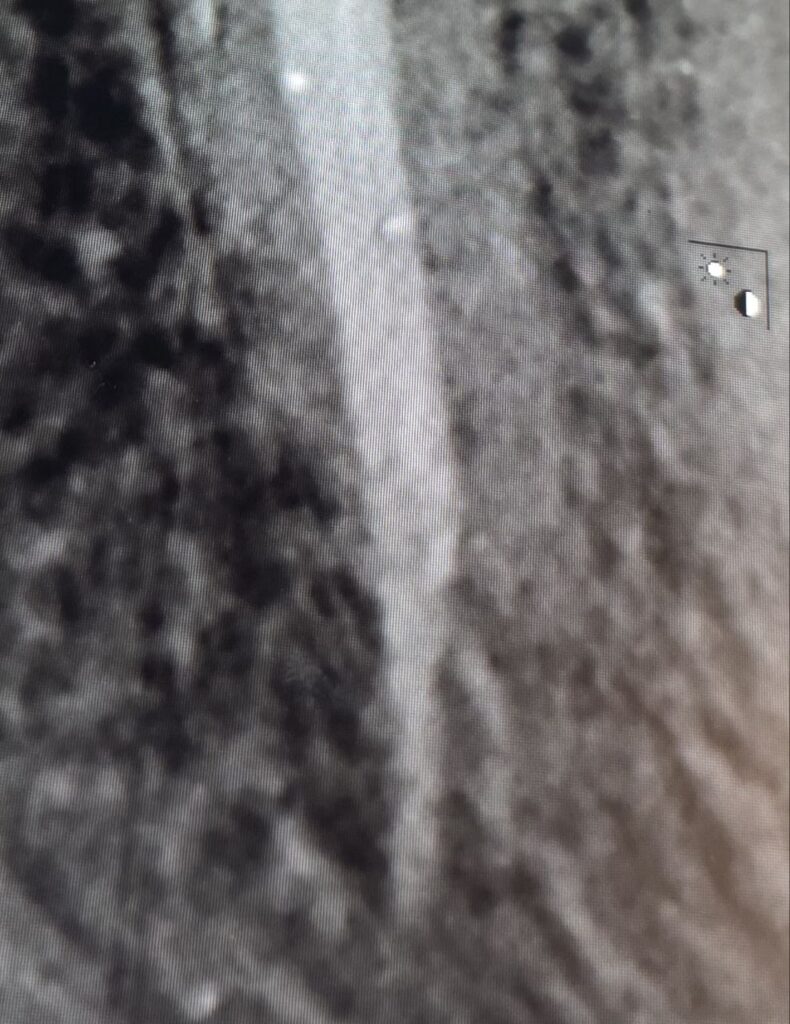
straight xray view of the upper shows lateral opening of the main canals or deep split

master cone xray view shows how complex it is before obt
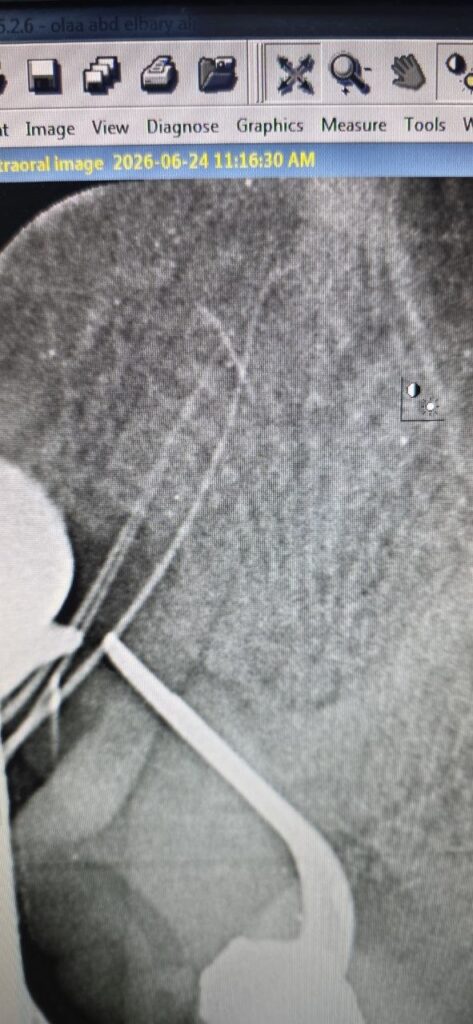
10k file
Share on: