A new case by our Zerodonto group expert Dr. Vincenzo Vitale
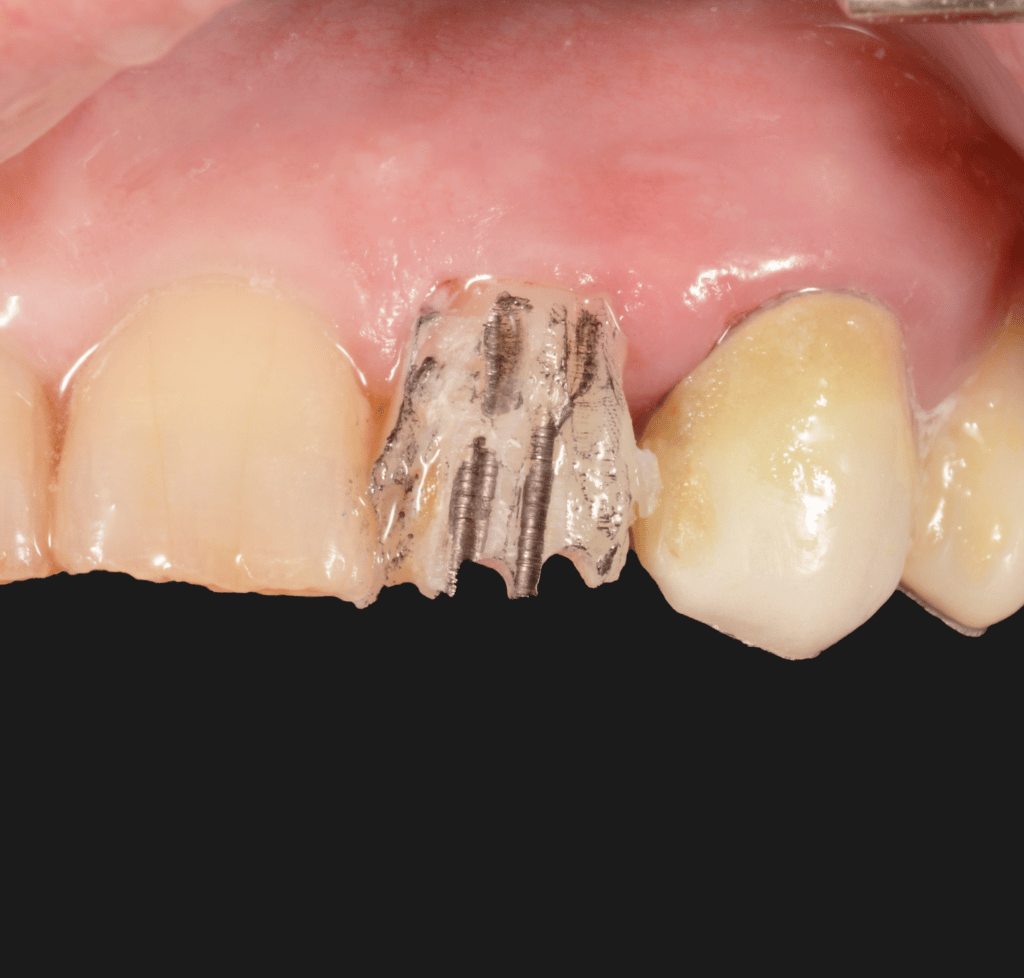
Patient came to our attention with a 2.2 fractured by trauma.
Clinical tests reveal: Vitality test: negative ; Percussion test: positive.
Due to severe evidence of abrasion and bruxism, the treatment plan proposed is:
root canal treatment of 2.2, buildup and zirconia crown.
The endodontic treatment is performed with martensitic Niti instruments and obturated with single cone and Bioceramic sealer.
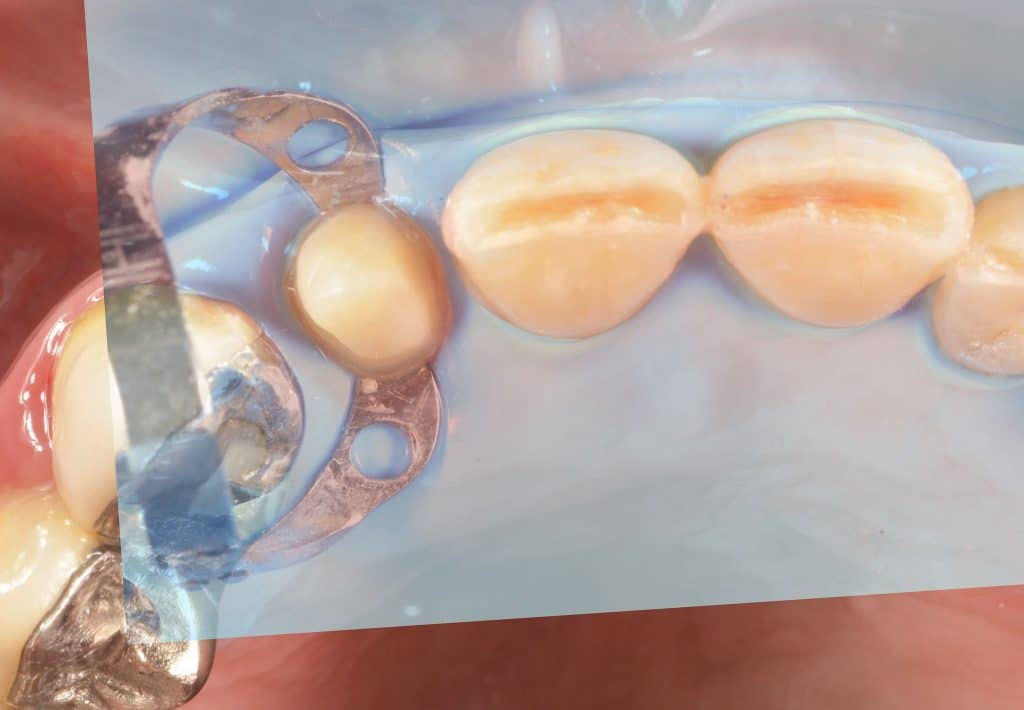
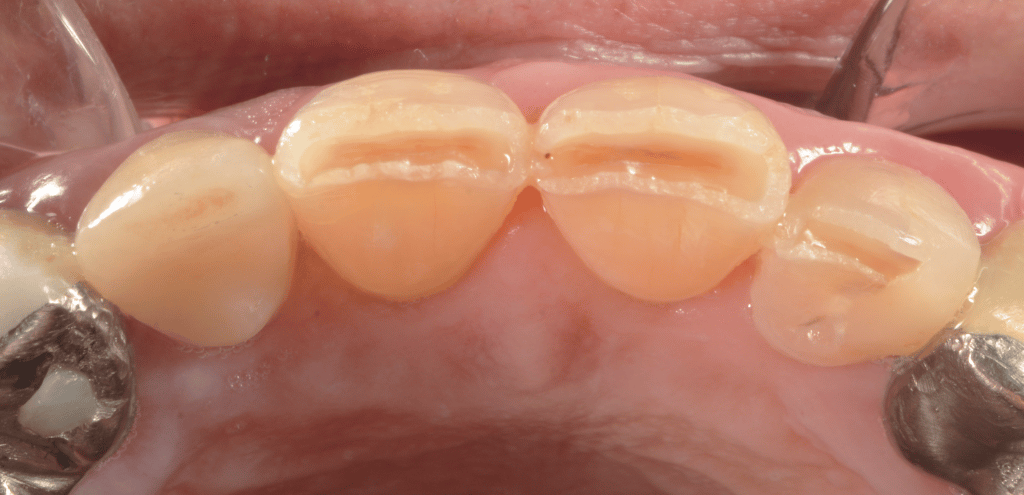
using Hawe steel matrix bands as scaffold, a build up is performed with flowable and packable composite. To increase the stabilization of the latter is used liquid rubberdam.
The build up must recreate a draft of morfology and volume of the final restoration to achieve a sort of mockup that can guide the calibrated preparation.
The preparation starts with calibrated depth grooves following the Kuwata inclined planes. To increase the precision in this phase, the depth of bur grovees are marked with a pencil and subsequently prepared.
A final champfer preparation is obtained with a subgingival margin of 0.5mm.
During the prep great attention is given to soft tissues.
With a 000 retraction cord the prep is finished slightly under the sulcus.
No bleeding is present and an immediate, final impression can be obtained using single phase putty and light Polyether impression material.
A resin provvisional crown is luted with temporary cement.
At the delivery the provissional is removed. Tissues are healty and, again, no bleeding is present.
Absolute isolation is achived with rubber dam and b4 clamp and teflon. (To learn more and some tips and tricks about absolute isolation check the article: https://www.myzerodonto.com/6-tips-and-tricks-for-your-rubberdam-isolation/ ).
APC protocol is used for adhesive luting of Zirconia.
A pretreatment that of Zirconia consists in an internal air-abresion with Al Oxide 50um at 2 bar pressure for 10/20 sec. .
Application of MDP primer and bonding not lightcured.
The tooth is cleaned, etched with 37% H3PO4 for 15/20 sec, water rinsed and uncured bonding application is performed.
With a self-adhesive resin cement the crown is seated. Meticolous removal of excesses and a lightcuing of 60 sec. on each surface is performed. Last lighcuring is carried out under Glicerine gel to allow curing of superficial inhibited oxigen layer of resin cement.
Rubberdam is later dissambled and occlusion is checked.
The final restoration, at control, shows a great integration with either soft tissues and teeth.

Isolated fractured tooth

fracture and martix scaffold

morphologic build up
prep with depth grooves

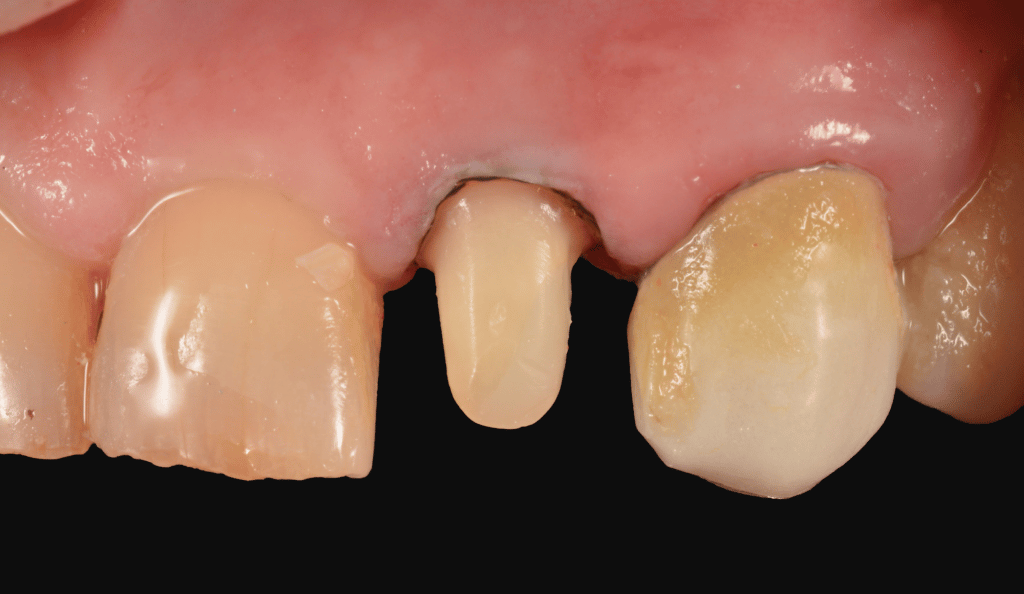
prep finishing

final impression

provisional phase

removal of provisional for delivery
isolation transition

isolation transition

isolation transition

absolute isolation

absolute isolation

absolute isolation

try-in

Anatomy of crown

Anatomy and color

etched
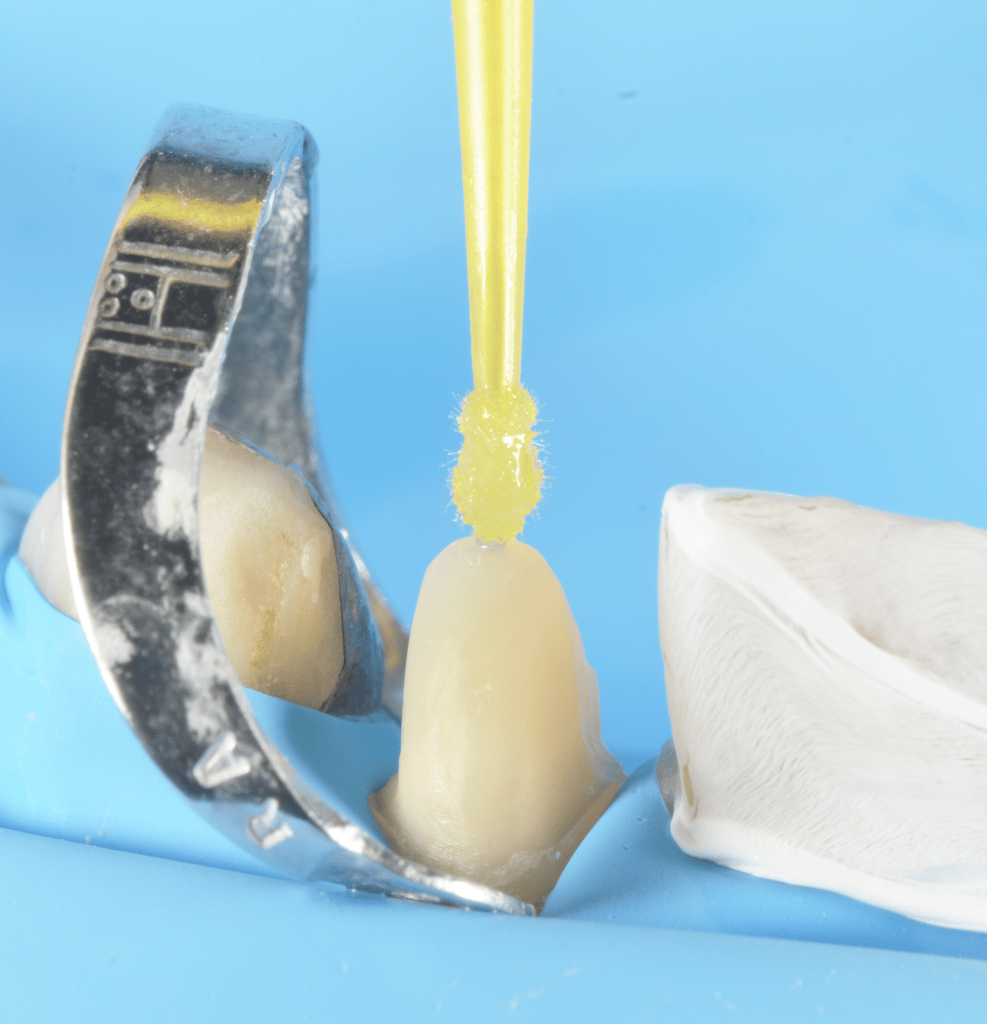
bonding

bonding

glicerine curing

final

smile

lateral
occlusal

pre and post
Share on: