Abstract:
The aim of this research is primarily to find and compare the accuracy of measuring working length with different types of electronic devices (electronic apex locators) and comparing it with the actual length of the root canal (the distance from the coronal reference point to an apical reference point 0.5 to 1.0 mm).
During the research, we relied on 9 healthy and integrated human teeth with one root and two roots that were obtained for this research from the clinics of our fellow dentists, specializing in orthodontics.
And we used 6 different devices of leading commercial companies in the market to make a comparison between them and to find the differences between those companies within the market. It was concluded that there was no statistical difference between the measurements of these companies.
INTRODUCTION:
One of the basics during the treatment of root fillings is to determine the length of the root.
(the root Working length) is defined as “the distance from a coronal reference point to an apical reference point (apical stop, apical constriction or narrowest apical diameter)
Based on this length, the channel will be prepared and expanded by files and reamers.
If we want to define (the apical constriction)Fig(1). It is most frequently located 0.5 to 1.0 mm short of the radiographic apex, but with variations.
The radiographic apex) is the tip or end of the root determined radio graphically Fig (2).
One of the tasks of finding the length of the canal and measuring it accurately is that this measurement will give you knowledge of the extent of the length based on which tools will be inserted to remove tissue and debris inside the canal, in addition to that it will give you full knowledge of the extent of measuring the canal filling in addition to the fact that it will affect the patient If there is an increase, decrease, or inaccuracy in measuring the filling or working length of the root, as the patient will sometimes feel pain or discomfort with the appearance of the ulcer or abscess, if there is an increase in the measurement of the length of the canal, for example, as something from the lack of correct measurement of the length The canal means that the root canal treatment will be unsuccessful.
Materials and method :
Sample collection:
We used 9 sound teeth (fully formed teeth) without caries, fracture, or any of the interventions in dentistry with one root and two roots from human teeth. Fig (3)
(Premolars) and they were hard collected from dental clinics, health centers, and most of our fellow dentists specializing in orthodontics within the current study and for its purposes.
We cleaned the outer surface of the teeth and rinsed them well to remove the remnants of adherent blood and surrounding tissues attached to the teeth. We did not take photographic rays, due to the lack of research time. We only used this option with the teeth with which we faced difficulty in readings.
The teeth were well examined under the light.
The teeth were without any defect and of similar size and appropriate to the type of research and the tools used within the research procedures. We numbered them and stored them in small cans in distilled water for the duration of the research. These cans were numbered separately and stored at room temperature.
Sample preparation:
Access cavity was prepared for each tooth using a high-speed turbine with sufficient water cooling
After we finished preparing the cavity, the tissue was withdrawn from the canal by a barbed broach. Fig (4)
the canal was checked with #15 stainless steel K-file (Dentsply company) without any preparation of the canal. Fig (5)
Working length masuremant :
The measurement of the actual length of the root canals was done by K-file (8,10,15) by Dentsply.
The files were first entered to find the clinical measurement, where the method of work was to insert the file towards the apical end of the root, where the end of the edge of the file could be seen with the naked eye from the apical hole of the root, then we adjusted the rubber stopper near the reference point (the tip of the buccal cups) where the final length was adopted as the length Clinical. Fig (6)
After completing the clinical length measurements as shown in the first field of Table 1. We used the electronic measurement, where samples were immersed in a plastic mold filled with a mixture of alginate Fig (7)(where alginate represents the mimic medium for the oral tissues surrounding the teeth).
of the electrodes of the electrical circuit. The readings were obtained at varying intervals as the devices relied upon within the research were not at hand.
Whereas the fifth generation Woodpecker device was owned by one of the students. Fig (8)
As for the third generation Woodpecker device, it is owned by the private Siwak Specialized Center in Babylon .Fig (9)
As for the Nano Eat device, it was owned by the private clinics of Capital, owned by its owner, Dr. Uday Al-Asadi. Fig(10)
As for the ipex 1 device, it belonged to the clinics of the College of Dentistry, University of Babylon.Fig (11)
And my device, Epex , for the two pediatric clinics and root fillings in the first specialized center of Babylon Governmental. Fig (12),(13).
In the first, it took us two to three hours, in the second an hour, in the third, two hours, in the fourth, half an hour, in the fifth, an hour, and the sixth hour, with the change of alginate material between every half hour to maintain the amount of moisture. The oral hook was kept in contact with the wet alginate during the period. Fig (14)
readings. We returned the readings for some devices once and twice, and the reading time for one tooth lasted from 5 to 20 seconds or more, with the readings decreasing or increasing during progress and withdrawal from the channel respectively. Fig (15)
All the measurements were recorded and organized in a table (Table 1). Fig (16)
For comparison of the accuracy of apex locators used in the current study, a non-parametric test was used (Kruskal Wallis test) Fig (17) with chi-square to test the significance between groups.
The result :
From the cumulative experience using the apex locators in the current study, it has been noted that measurements with Nano Est were a lot easier than other devices, while the measurements with (iPexI) were the most difficult ones. Results obtained from the current study were organized in Table 1. It has been found that readings from the (iPexI) were the least accurate among all devices with very close results between the iPexI and iPexII. The mean and standard error for all groups were listed in Table 2.
It was determined that each sample was regarded as its control. Statistical analysis revealed a non-significant difference among the devices used in the current study regarding their ability to determine the accurate working length (P≤0.05) as can be seen in Table 3. Undoubtedly, working length estimation is a crucial step in successful endodontic treatment, where instrumentation and obturation beyond or short of the apex will dramatically worsen the scenario and lead to endodontic treatment with a poor prognosis. The experimental model utilized in the current study is a modified model from a study by Leonardo, where the immersed samples can provide a close electrical resistance to that of the periodontal tissues. Furthermore, this model is simple, readily available, easily manipulated, and provides firm control for the experimental variables to be tested but it has the drawback of incomplete simulation of the patient condition.
Apex locators are regarded as a precious addition to the world of endodontics , where the newly introduced devices can detect the exact point where the periodontium starts at the end of the canal. It has been reported that the accuracy of some apex locators was 100% accurate within ±1.
0 mm and from 75-91.7% accurate within ±0.5mm in simulated dry canals, whereas a dramatic decrease in the accuracy was reported with the increase in simulated canal diameter. Several studies focused on the accuracy of apex locators and produced comparable results with accuracy of around 80% within ±0.5 mm and almost 100% within ±1.0 mm,. The majority of researchers considered the error range acceptable at ±0.5mm and fewer researchers considered ±1.0mm. This was due to the great variability in the shape of the apical area in addition to the fact that it is somewhat difficult to visually control the distance between the reference point and the rubber stopper. Furthermore, it is tricky to detect the exact point where the tip of the reamer exit the canal regardless of the magnification used. In the current study, both error ranges were adopted. Although the non-significant difference was reported in the current study, the devices show some easily detected differences.
Statistically, woodpecker GV was the most accurate device (76.5% within ±0.5mm and 100% within ±1.0mm) compared to clinical measurements with the (iPexI) being the least accurate one (17% within ±0.5mm and 67.6% within ±1.0mm). Despite the statistical results which showed that the woodpecker GV is the most accurate, its mean value is
more than the clinical mean value. So, the most accurate reading was with Nano Est. Within the limitations of the current study, it can be concluded that apex locators are valuable devices for the working length determination with an accuracy of up to 100%, and Nano Est was the most accurate than woodpecker GV , then woodpecker GIII , ePex China , ePex Germany , with the iPexI was the least accurate with a statistically non-significant difference.
Conclusion:
Within the limitations of the current study, it can be concluded that apex locators are valuable devices for working length determination with an accuracy of up to 100%. Through this study, it was found that there is no statistical difference between the measurements of these companies, despite a very small difference between the readings that may not be taken into account. It was noticed that the Nano Est was the most accurate, while the iPexI was the least accurate, with a statistically non-significant difference.
It is recommended to conduct a future study on a larger number of samples and compare the working length of the root canals using the same devices used in this study or more additional devices.

Fig (14)

Fig (1)

Fig (15)

Fig (16)
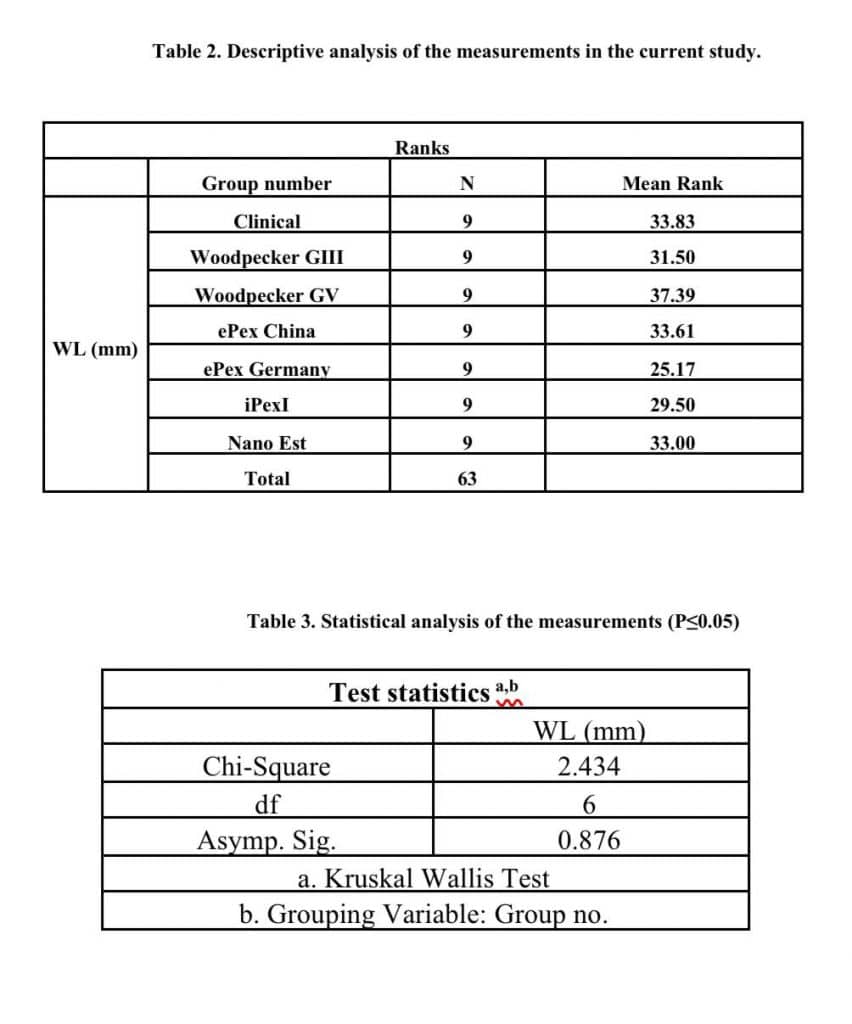
Fig (17)
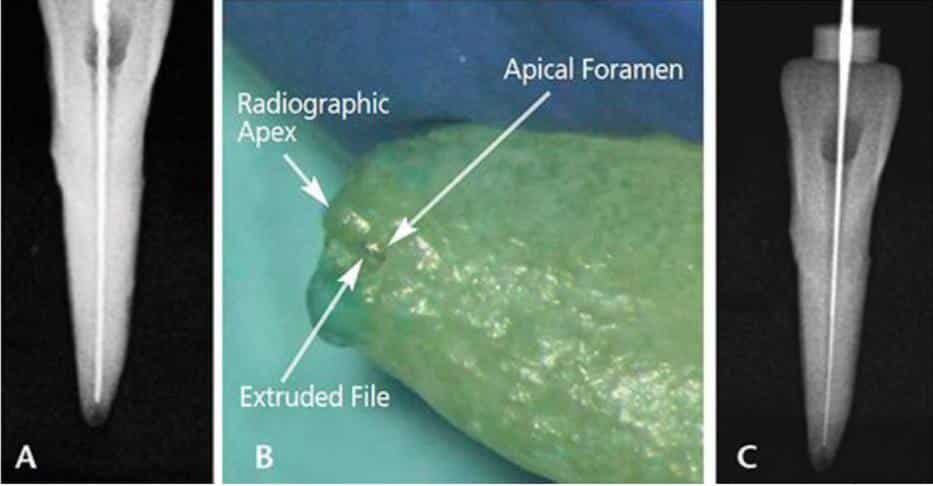
Fig (2)

Fig (3)
Fig (4)

Fig (5)
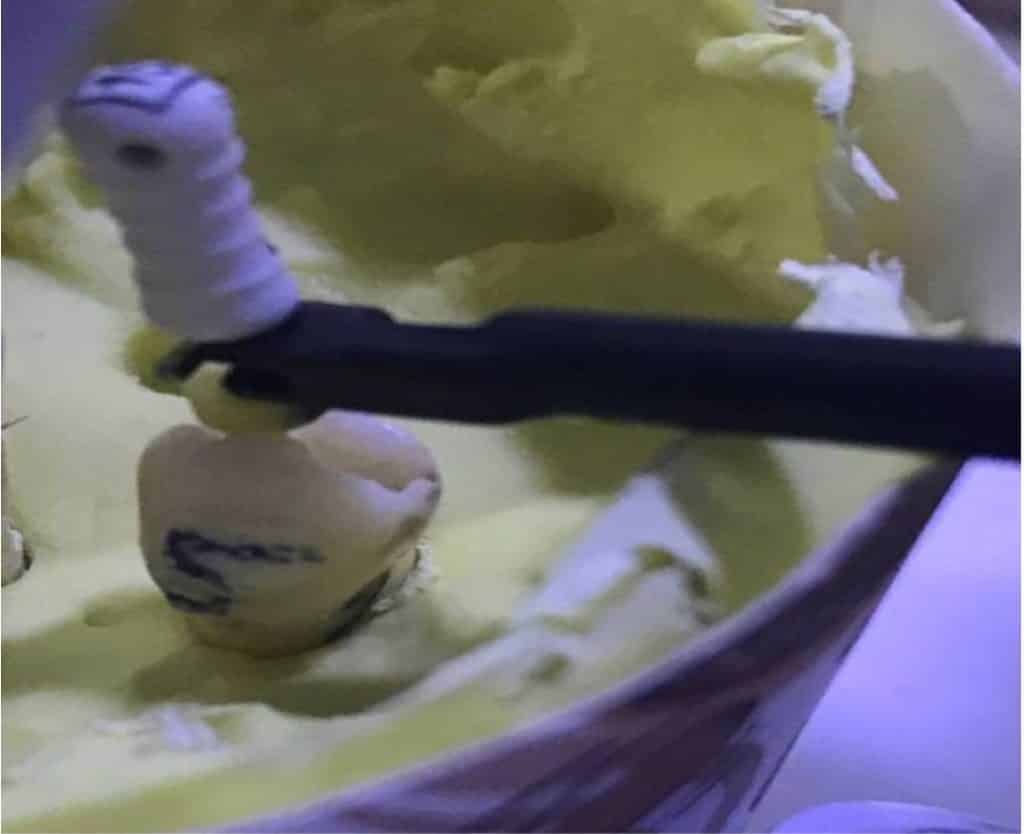
Fig (6)

Fig (7)
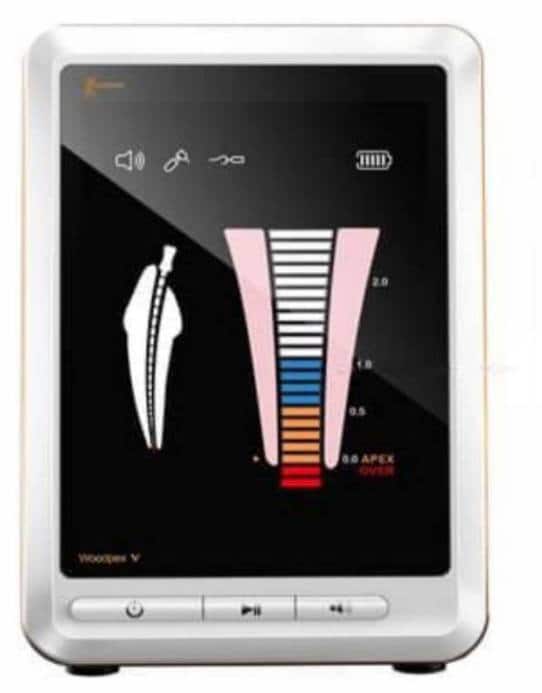
Fig (8)
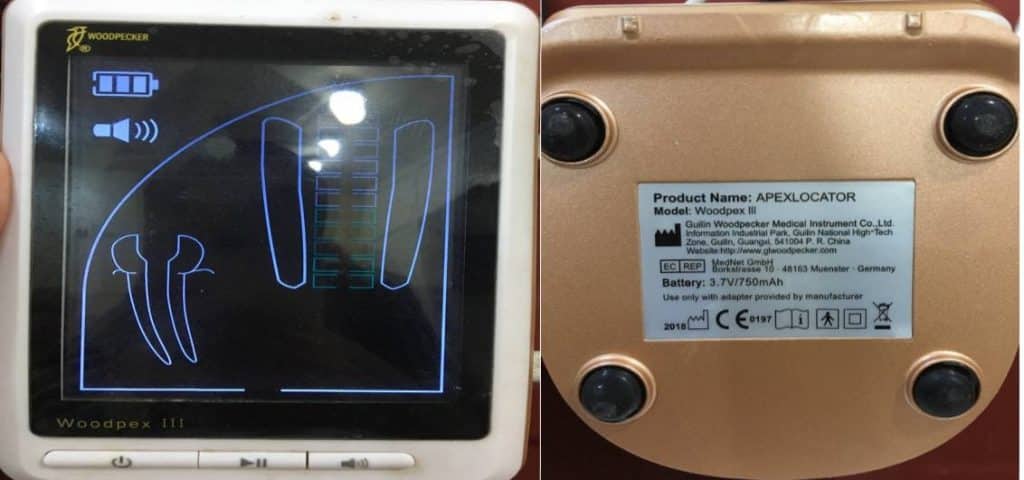
Fig (9)

Fig (10)

Fig (11)

Share on: