A case from our community member Dr. Vincenzo Vitale
The Pulp vital thepary (PVT) is an alternative procedure to root canal treatment for teeth that have received pulp exposure due to trauma or a carious process.
This procedure consists in the application of a material over the exposed pulp able to preserve its vitality.
In literature there are several materials tested and proposed, all with one goal; to promote the dentinogenic potential of pulp cells to maintain the vitality of the tooth.
The main indications for this type of therapy are:
1. Permanent and temporary teeth with persistently mechanically or traumatically pulp
2. No history of spontaneous or irreversible pulpitis
3. Vital pulp
4. Absence of periapical radiographic lesions
5. Controlled pulp bleeding. (1)
In this article we will describe a case of PVT treated with a bioceramic material.
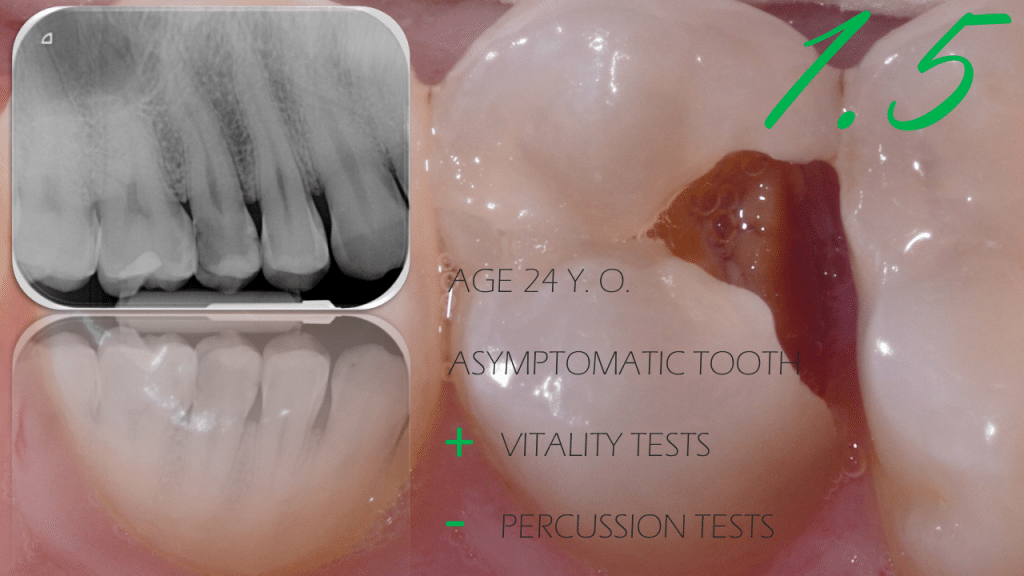
The patient, 23 Y.O. , presented for clinical inspection with asymptomatic distal destructive caries on right second upper premolar.
At the bitewing examination mesial and distal radiotranslucency with intimate pulp contact is noted.
After the anesthesia, the rubber dam is mounted and the dentinal carious tissue removed by means of a tungsten carbide round bur mounted on a micromotor.
With a green coded round diamond bur the undermined enamel is removed and the buccal and palatal cusps are reduced, in anticipation of a future overlay.
During the removal of the carious tissue, the exposures and bleeding of the two pulp horns are noted.
Once the cavity cleansing has been completed, an automatrix is mounted to proceed with the haemostasis and cleansing protocol for the subsequent application of the bioceramic material (2).
Bleeding is controlled by using sterile cotton wool balls soaked in 5.25% sodium hypochlorite.
After about five minutes the bleeding is stopped and a new cleansing is carried out with cotton wool soaked in physiological solution.
A final cleansing involves the use of Edta only 17% to allow the bioceramic material to better penetrate inside the dentinal tubules (3).
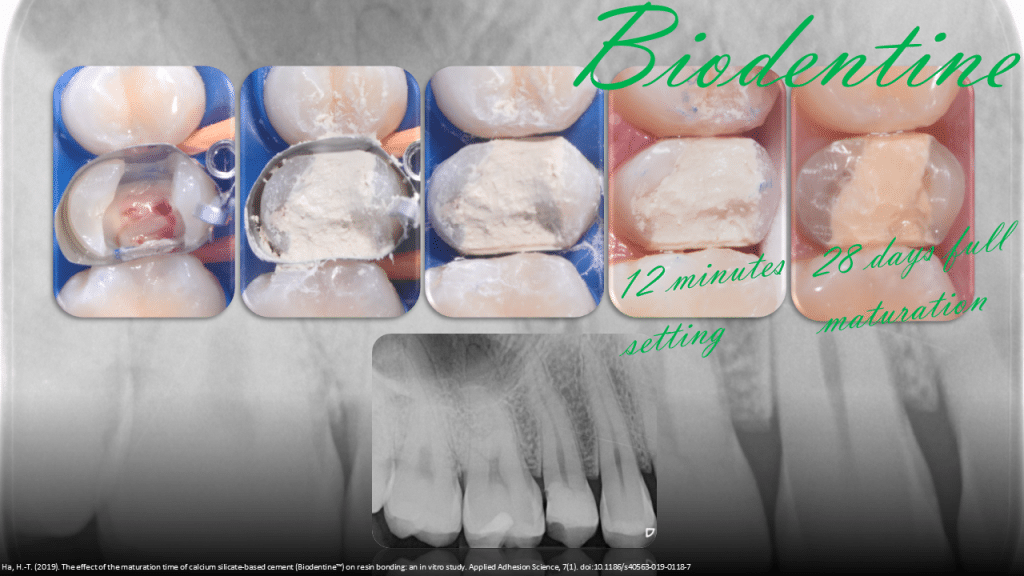
The application takes place in small increments until the dental defect is filled.
After 12 minutes for the material to polymerize, the dam is disassembled and checked that the element is free from occlusion.
The patient is sent back to carry out the preparation and restoration after at least 28 days, thus allowing Biodentine to reach complete maturation, which gives valid Compressive Strength (300MPa) and Shear Bond Strength values to withstand occlusal loads and allow correct adhesion (2,4,5,6).
The patient is checked after a week and reports that he has no discomfort but only a slight tenderness of the tooth in question (as expected).
After about a month, the patient come back.
The rubber dam is mounted, the preparation is carried out with diamond burs, treating the bioceramic material as if it were dentin.
During the preparation, attention is paid to having a 360 ° enamel cerclage. The cusps that have a thickness at the base <2 mm are reduced and a palatal butt joint and a vestibular bevel are performed, creating a non-retentive preparation (7,8).
Once the shade has been detected using the Vitapan classic scale, an intraoral scan is carried out and the VitaEnamic hybrid ceramic overlay is designed and milled.
The adhesive phases involve selective etching of the enamel followed by a self etch technique on Biodentine and enamel (4).
The hybrid ceramic framework is cemented with heated restorative composite (8).
Clinical and radiographic control at three months showed no alterations. The tooth responds normally to vitality tests and the restoration has excellent integration.
The element will be monitored with periodic follow-ups.
Bibliography
1.Cohenca, N., Paranjpe, A., & Berg, J. (2013). Vital Pulp Therapy. Dental Clinics of North America, 57(1), 59–73. doi:10.1016/j.cden.2012.09.004
- Bachoo IK, Seymour D, Brunton P. A biocompatible and bioactive replacement for dentine: is this a reality? The properties and uses of a novel calcium-based cement. Br Dent J. 2013 Jan;214(2):E5.
- Harik R, Salameh Z, Habchi R, Camilleri J. The effect of irrigation with EDTA on calcium-based root canal sealers: a SEM-EDS and XRD study. J Leb Dent Assoc. 2016;49:12–23.
- Odabaş ME, Bani M, Tirali RE. Shear bond strengths of different adhesive systems to biodentine. ScientificWorldJournal. 2013 Oct 10;2013:626103.
- Ha, HT. The effect of the maturation time of calcium silicate-based cement (Biodentine) on resin bonding: an in vitro study. Appl Adhes Sci 7, 1 (2019).
- Krawczyk-Stuss M, Nowak J, Bołtacz-Rzepkowska E. Bond strength of Biodentine to a resin-based composite at various acid etching times and with different adhesive strategies. Dent Med Probl. 2019 Jan-Mar;56(1):39-44.
- Politano G, Van Meerbeek B, Peumans M. Nonretentive Bonded Ceramic Partial Crowns: Concept and Simplified Protocol for Long-lasting Dental Restorations. J Adhes Dent. 2018;20(6):495-510.
- Ferraris F. Posterior indirect adhesive restorations (PIAR): preparation designs and adhesthetics clinical protocol. Int J Esthet Dent. 2017;12(4):482-502. PMID: 28983533.
- Magne P, Razaghy M, Carvalho MA, Soares LM. Luting of inlays, onlays, and overlays with preheated restorative composite resin does not prevent seating accuracy. Int J Esthet Dent. 2018;13(3):318-332. PMID: 30073216.
Time 0

Excavation of decay exposing pulp
Hemostasis control and Biodentine application
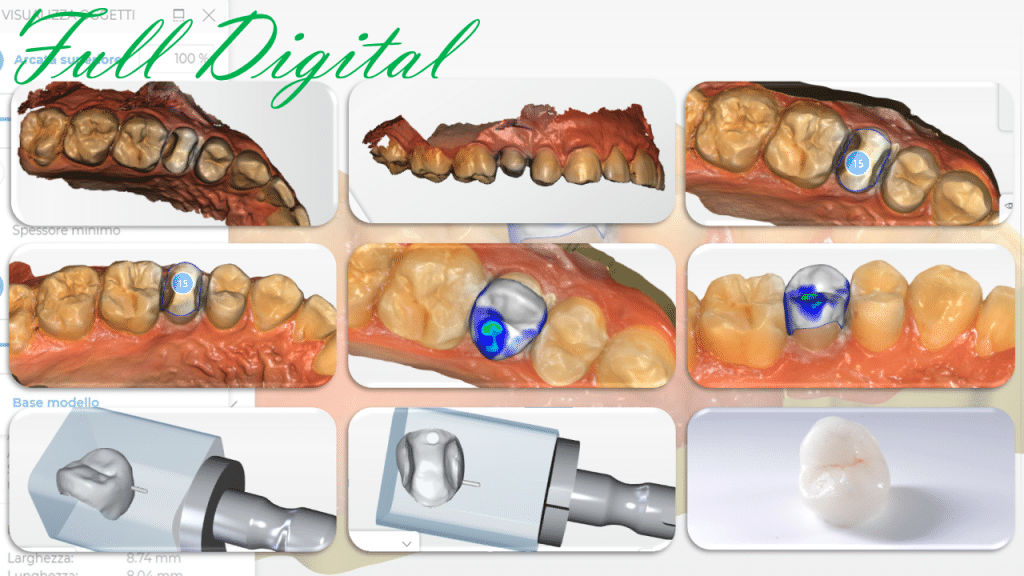
Full digital protocol

Adhesion using Selective enamel etching with 37% ortophosforic acid + SE adhesive. Overlay luted with warm composite restorative material.
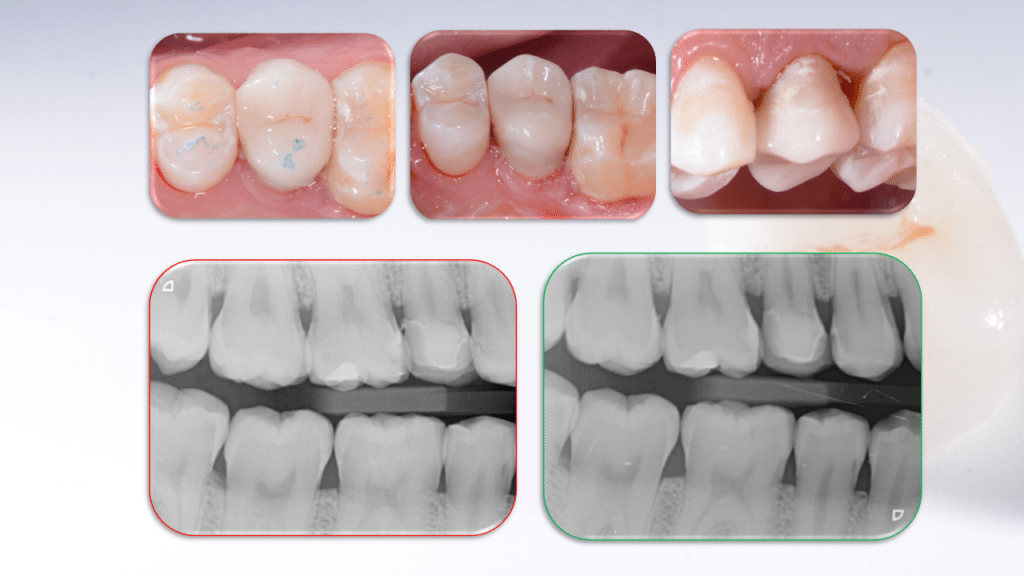
Immediate post op. Always check radiography

3 months control.
Share on: