
- The first and most important thing in any procedure, adult or pediatric patients, and what will determine the procedure; is your diagnosis .. In Pediatric dentistry, the diagnosis can determine if you will go to pulpotomy or pulpectomy.
- If the pain Momentary Pain and it comes only while eating, cold water or sweets and goes away, we are reversible pulpitis stage .. so you are understanding the possibility of pulpotomy
- If the pain is continuous, its indication of wide spread inflammation reaching the radicular pulp tissue, and here we in irreversible pulpitis stage , and we at possibility of partial pulpectomy or pulpectomy
- If the pain is Spontaneous, throbbing and constant and it occurs especially at night, its indication of progressive or extensive degeneration of the pulp, and here we are sure that we go to pulpectomy
- Clinical examination:
1- Pain with percussion: it is indication for periodontal ligaments inflammation, applying your finger with pressure to the tooth and
check the child's response, here we will also go to the pulpectomy; unless there is a physiologic resorption in primary tooth due to eruption of permanent one.
2- If you find swelling related to the tooth, intraoral or extraoral, or fistula, in this case, it will be non-vital, Confirm your diagnosis with x-ray to see whether root resorption has occurred or not; If not, go to pulpectomy
3- If you find mobility in the tooth, it may be physiologic or may be due to any persisting pathology.
Of course, you must take a pre-operative x ray to confirm your diagnosis.
- Ok, so you knew that before starting procedure that you will go to pulpotomy or pulpectomy. But, if you still don't know, and all you know is that you are going to do pulp therapy, What do you do?

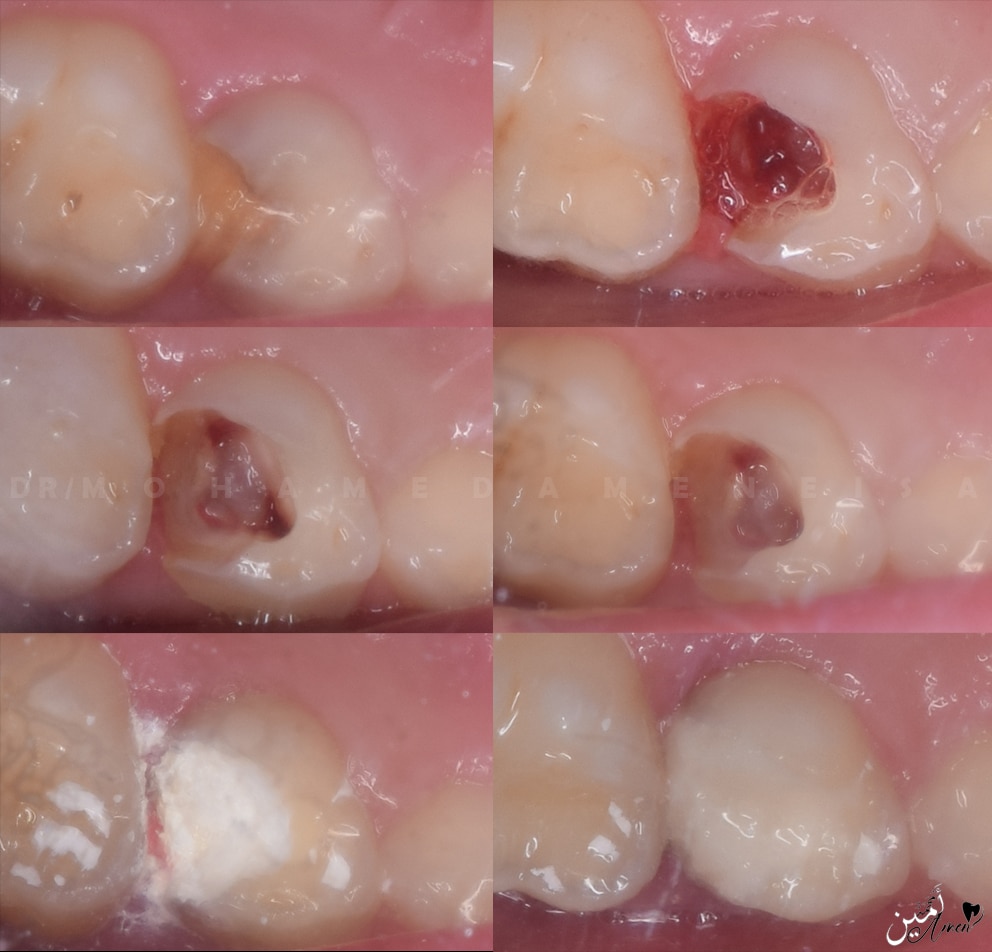
- Starting open access with large round bur to feel with the drop and to avoid perforation in the pulpal floor, after the drop you start deroofing, You can use endo Z bur here, and you can complete with large round bur.
- You should do complete deroofing to locate the canals..

- After completely deroofing, start to remove the coronal pulp tissue with a large round bur or sharp excavator, but it is preferable to use a sharp excavator to avoid perforation
- Remove all coronal inflamed pulp tissue, especially above the canals, to remove all inflamed pulp tissue.

- Stop bleeding and achieve hemostasis by using cotton pellet with saline in the cavity for 5 minutes
- If bleeding has stopped, it is indication that the inflammation is constricted to coronal pulp tissue and go to pulpotomy, If not stop, you have two possibilities:
The first possibility: is that you dont remove all inflammed coronal pulp tissue and there is still inflamed tissue above canals orifices. So you will back to remove this inflammed tissue and get another cotton pellet and put it again for 5 min. and see
The second possibility: that the inflammation reached radicular pulp tissue, and in this case you will go to pulpectomy.
If you are sure that you have removed all of the inflammed coronal pulp tissue and it is still bleeding, go for a pulpectomy directly
- Do not use a cotton pellet with formocresol to stop bleeding, the bleeding will stop, but this is a fake hemostasis, so it is not possible, the blood should stop alone with a cotton pellet with water or saline, not with formocresol

- The blood stopped, and you decided to do a pulpotomy; You can use the best of the two methods, but the second is better and you will know why
1- Devitalization technique
- In this technique, you take a cotton pellet with formocresol (you just sniff the cotton pellet with formocresol and squeeze it into another dry cotton pellet, because formocresol works with its fumes) and put it in the cavity for 5 minutes, and when you remove the cotton from the cavity, the pulp tissue of orifices appears as dark brown or black, and this is an indication that the pulp has been fixed
- But; the formocresol mummifies all the pulp, and creates local toxicity, In addition to that; formocresol is absorbed into the systemic circulation from the pulpotomy site with a cytogenetic and mutagenic effect.
Formocresol harms the succedaneous teeth because it spreads through the apical foramen, which a high risk of enamel defects in the permanent successor. Therefore, we will go to second technique.
2- Preservation technique
Here, instead of using formocresol, you can use ferric sulfate or sodium hypochlorite, and the easiest and cheapest one is sodium hypochlorite.
- You take a piece of cotton and soak it in sodium hypochlorite and put it in the cavity for 30 seconds, Here you have preserved the radicular pulp vitality, and it will give you the fixation you want without the harm of formocresol
I will remind you that you do these steps after you are 100% sure that the bleeding has stopped.

- The blood stopped, fixation layer achieved, so, you start to apply the ZOE by making a thick mix, that you can handling it like temporary filing
- You put it layer by layer, and you take a piece of cotton soaked in water and squeeze it well and hold it with a tweezer, and press comfortably on the ZOE like doing condensation, then you put the next layer on and do the same thing for another time, keep the last 4 mm for final restoration.

- If you will make SS crown, you can fill the cavity with ZOE and place the SS crown as final restoration.
- Or put a layer of the ZOE then layer of GI then SS crown
- If you will not make SS crown, put a layer of ZOE, then amalgam or composite,
- If you going to composite, you can't put it directly on the ZOE because the eugenol can inhibit the polymerization of the composite, so we have to put base which is the glass ionomer, then composite restoration
- if you going to amalgam, put layer of ZOE then Layer of zinc poly carboxylate as base then amalgam
Here I put ZOE and a glass ionomer on it to make an SS crown.

Thank you for reading
