Case presentation:
-45 years old female patient came to our clinic complaining from sensitivity with hot & cold regarding lower 2 central incisors area.
-The patient is systemically free and had no drug history.
Clinical examination:
-Clinically there were many observations:-
1-Marginal gingival recession was noted in lower 2 central incisors.
2-Interdental papillary loss between the 2 central incisors especially in the mesial aspects due to interdental attachment loss.
3-Spacing between central incisors & lateral incisors but it was more between the 2 central incisors.
4-Slight rotation of the 2 central incisors.
5-Very thin gingival phenotype or biotype (tissue thickness) which is one of the risk factors for gingival recession. “Note that the microvasculature was apparent in the whole alveolar mucosa”.
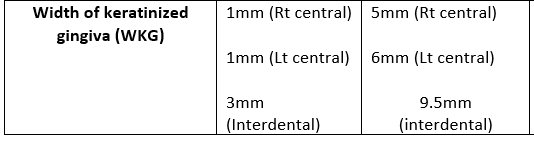
6-Very narrow zone of keratinized tissue especially all around the 2 central incisors. “almost 1mm from the free gingival margin to the mucogingival junction”.
7-Ginigva is inflamed due to presence of local irritants “calculus deposits” adherent on the proximal surfaces of both central incisors.
8-Positive fremitus test (+1) which meant that the 2 centrals were under trauma from occlusion.
-Periodontal chart measurements for the 2 central incisors:-
-As shown in the figure. “Check the photos”
Treatment plan:
-It was very important to rule out the exact cause of gingival recession related to the 2 centrals before putting the appropriate treatment plan for the case.
-According to Miller classification , This case was classified as Miller class III as marginal tissue recession here extends to mucogingival junction “MGJ” leaving a insufficient keratinized tissue
“ 1mm “ together with interdental tissue loss due to interdental alveolar bone loss which was observed on x-ray as shown in the photos.
“mild horizontal bone loss as alveolar crest level is midway between cervical & middle thirds of both roots ”
-Orthodontic closure to eliminate spacing would add for sure on the prognosis of the case so the case was referred first to an orthodontist which reported that it is contraindicated for orthodontic treatment due to patient’s age and interdental alveolar bone loss which can’t be regenerated as it is “horizontal” .(no housing nor enough blood supply for the bone substitute material)
-So , first step was to eradicate all local irritants through scaling & curettage followed by occlusal adjustment to relief the 2 teeth from occlusal trauma. “Stop the cause”
-2nd step was to advance to the surgical technique for the root coverage, which was to choose to harvest a free gingival graft.
-The main aim of harvesting the free gingival graft is to:
1-Regain deficient keratinized tissues, thus modifying the thin phenotype of the gingiva into thick phenotype gaining future prevention against any further gingival recession.
2-Root coverage to eliminate root sensitivity for the patient although here we can not get full root coverage due that interproximal attachment loss is less than labial attachment loss & also due to interdental bone loss.
-Surgical procedure steps:-
1-In order for the free gingival graft to survive , regenerate the needed keratinized tissues & avoid its necrosis , a vascular bed was needed to be prepared on the recipient site to give the needed blood supply to the graft through blood vessels bridging between the grafted tissue and the vascular bed as exposed root surfaces are avascular & won’t give any blood supply .
2-The graft must cover at least 3mm of the vascular bed mesial , distal & apical to the exposed root surface…..so the vascular bed size should be bigger than the graft size.
3-3 split thickness horizontal incisions were made at the base of interdental papillae surrounding the 2 central incisors with 2 vertical incisions “ distal to distal papillae of both teeth”
4- 2 vertical incisions were made oblique in direction giving the chance to the vascular bed base to be wider than the top for better blood supply & they should extend apically (4-5) mm beyond mucogingival junction.
5-The strip of the epithelium was dissected revealing the underlying periosteum.
6-A template “ paper cover of Suture ” for example was used to measure the needed graft size on the exposed roots & vascular bed.
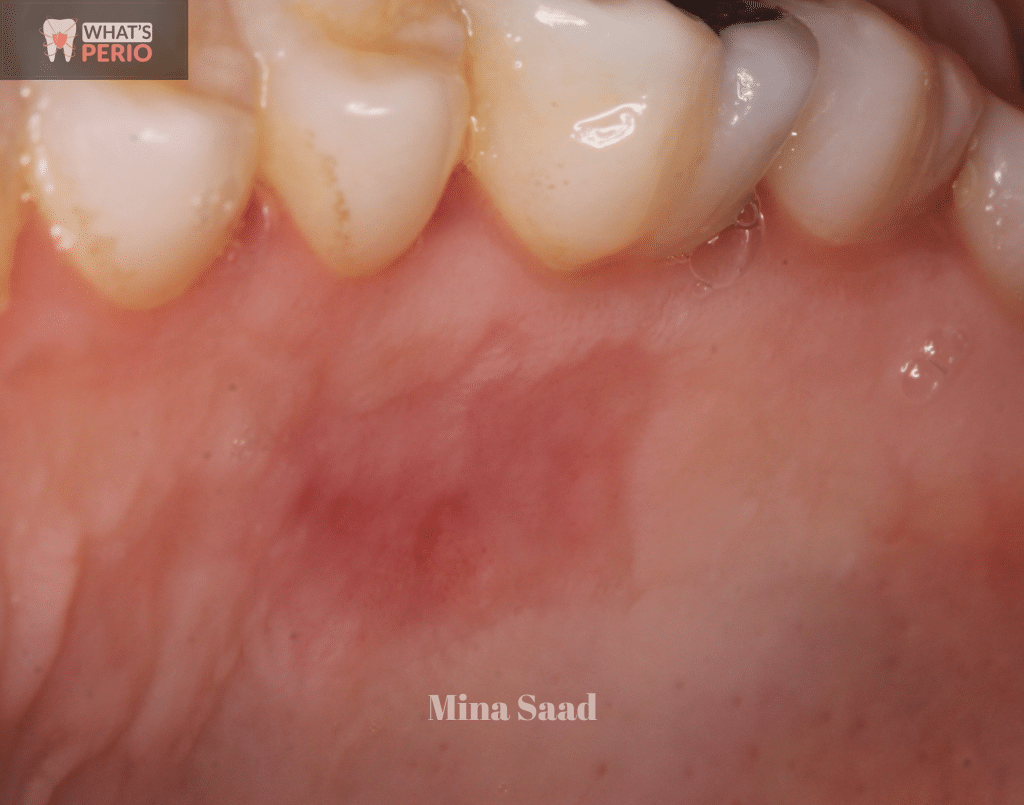
7-The graft was harvested from the hard palate “midway between the median palatine raphe & distal surface of the free gingival margin of upper canine”. (this to avoid rugae area as it had excessive adipose tissue which can impair the healing)
8-The template was placed over the required site for harvesting… 3mm away from the free gingival margins & 4 incisions were made all around the template. “2 horizontal , 2 vertical”
9-The graft was dissected & consisted of epithelium and underlying periosteum and should be 2mm even thickness.
10-Usually the palatal wound heals by 2ndry intention and underlying periosteum will favor keratinization.
11-A Piece of cotton soaked in a hemostatic solution “Kapron ampoule” (tranexamic acid) was applied over the wound to stop bleeding & an acrylic stent was placed over the wound to avoid its contamination and decrease pain sensation during healing period.
12-Mechanical root planning was made on the recipient site using curette followed by root conditioning using cotton pieces soaked in tetracycline solution placed over exposed root surfaces for 5 minutes followed by saline irrigation to wash out tetracycline.
13-The purpose of root planning & conditioning was to remove any remnant necrotic cementum exposing the healthy cementum which will be ready for attachment to the grafted tissue.
14- The acrylic stent was prepared 1 week before the surgery by taking impression to the upper arch & fabricating it on a model , it had 2 Adams clasps & short labial arch to maintain its stability……fitting surface of the stent especially over the donor site should have adequate space “ relief” to avoid any pressure on the wound……..it can be used also to apply topical medications like Gengigel “hyalouronic acid” on its fitting surface to accelerate wound healing.
15-Keep the graft always wet till adapting it over the recipient bed by immersion in saline or applying saline over the graft using a plastic syringe……anyway it should not be delayed to be placed over the vascular bed to maintain its vitality. “no more than 3 minutes”
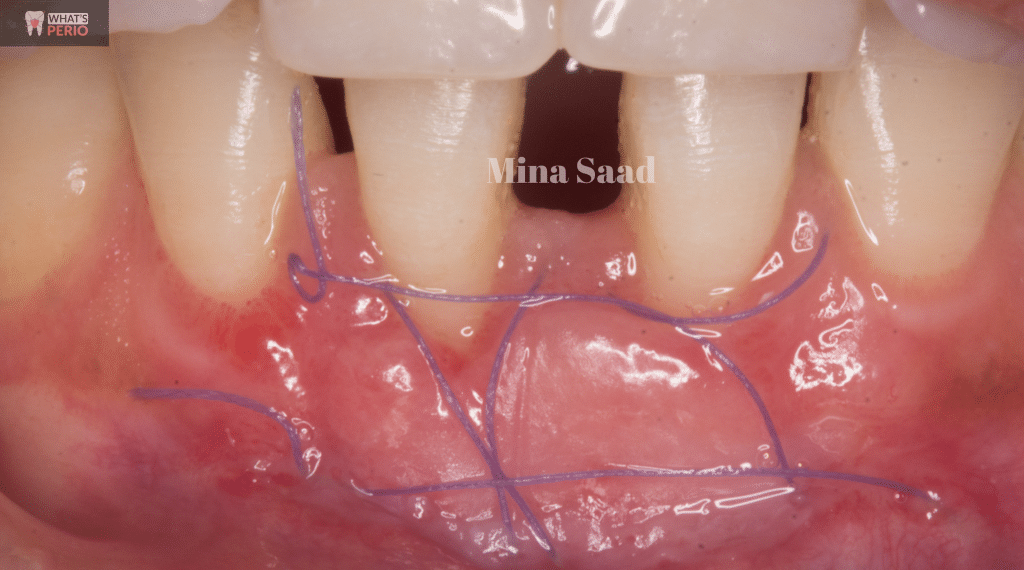
16-The graft is secured to the underlying periosteum using :
A-2 simple interrupted sutures mesially and distally.
B- 2 X-shaped or Criss cross sutures were made to secure & adapt the graft over the periosteum.
“compressing sutures anchored to the periosteum apical to the graft and suspended around
lingual cingulum “
(All sutures made are 6/0 resorbable vicryl “polyglycolic acid”)
-The purpose of mattress compression sutures :-
I-minimizing thickness of the clot that forms between the graft & root surface.
II-Ensuring that the coronal graft margin fits tightly over the root surfaces reducing both exposure of the clot & postsurgical shrinkage of the grafted tissue.
C-Horizontal periosteal sutures were made for fixation of the vestibular depth.
17-A periodontal dressing “Pericem” was applied over the recipient site.
18-The patient is instructed to remove the acrylic stent 1 hour after finishing
the procedure to make sure bleeding was stopped.
19-The patient was instructed to use the fitting surface of the stent to deliver gengigel over the donor site wound to accelerate healing.
“2 times per day for one week ……each time
the stent was put in place for 10 minutes”
19-The patient is instructed to:
A-Apply cold packs over the donor site & recipient site every hour for 10 minutes in the first 2 days.
B-The prescription included Hibiotic (1gm) , Cataflam (50 mg) & Alphintern….. to control post-operative infection, edema & pain.
C-Avoid hot & spicy food.
D-use a soft toothbrush and avoid eating or brushing in both sites.
20-the patient was called for follow up after 1 week.
21-After 1 week, the patient came to our clinic & the periodontal pack was removed…..revealing a whitish layer was formed on the external surface of the graft.
22-The donor site wound had a mixed color “red & white” which indicates that it started epithelization.
23-During this stage the patient is instructed to use antiseptic mouth wash “Chlorohexidine” frequently 2 times per day “Orovex” and still to avoid toothbrushing at the recipient site to avoid any interference with healing …and the patient was requested to follow up after 1 week
24-in the 2nd week follow up , the palatal wound was almost to be completely healed as it became pale red in color and epithelization increased….and there is no need for the stent now.
25-The recipient site revealed the appearance of thick , new tissue with pale pink color which indicated that the healing now is in the “re-epithelization stage”
“Note: as the time passes, the graft takes on the color & surface features of the palatal mucosa from which it is harvested”
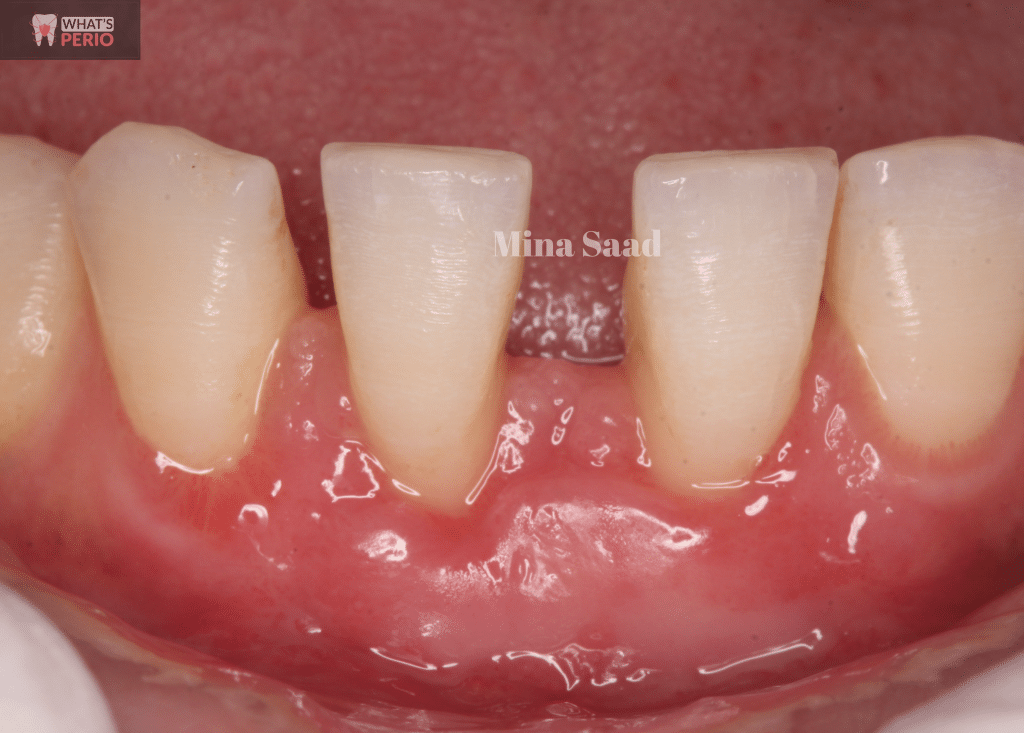
26- The patient was recalled for follow up over 5 months and the following observations were found:
A-With every month it was clear that the grafted tissue become thicker and more pale resembling more the color of palatal mucosa with marked color mismatch with the surrounding keratinized gingiva & unevenness of the mucogingival junction below the grafted tissue which of no clinical significance or disadvantage as the graft is in a non-esthetic zone.
B- there was significant decrease in Recession depth (RD) measurements & this occurs due to creeping attachment of the grafted tissue which is known as
post-operative migration of gingival marginal tissue in a coronal direction over portions of
a previously denuded root.
“Range of creeping was 1.5mm for right central & 1mm for left central”
C-Gaining more keratinized tissue all around the 2 central incisors.
(Right central= 1 mm at baseline, 5mm after 5 months)
(Left central = 1mm at baseline, 6mm after 5 months)
(Interdentally = 3mm at baseline, 9.5mm after 5 months)
27-Patient is asked to continue following the traditional oral hygiene measures with frequent follow up every 6 months.
Very much thanks to the lens of our talented photographer Dr Ragui Yousry Guirguis

Preoperative photo
Microvasculature is very apparent in alveolar mucosa

Recession depth (RD) for right central = 3 mm.
"RD is the distance between cemento-enamel junction (CEJ) & free gingival margin"

Recession depth (RD) for left central = 2 mm.

Preoperative chart measurements "Buccal"
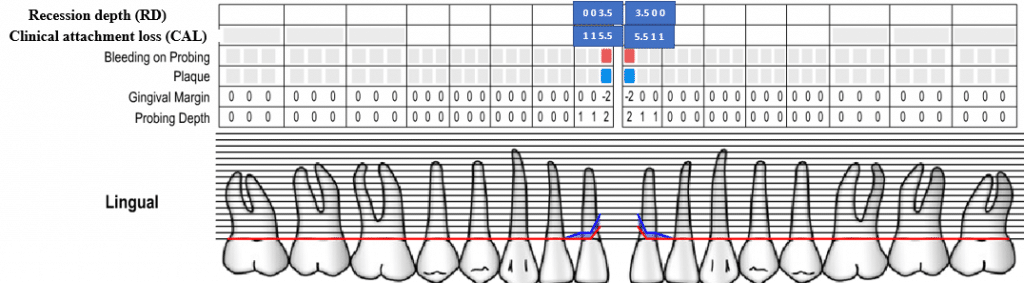
Preoperative chart measurements "Lingual"

Width of kerstinized gingiva (WKG).... The distance between free gingival margin & Muco-gingival junction (MGJ)

Mild horizontal bone loss between 2 centrals.
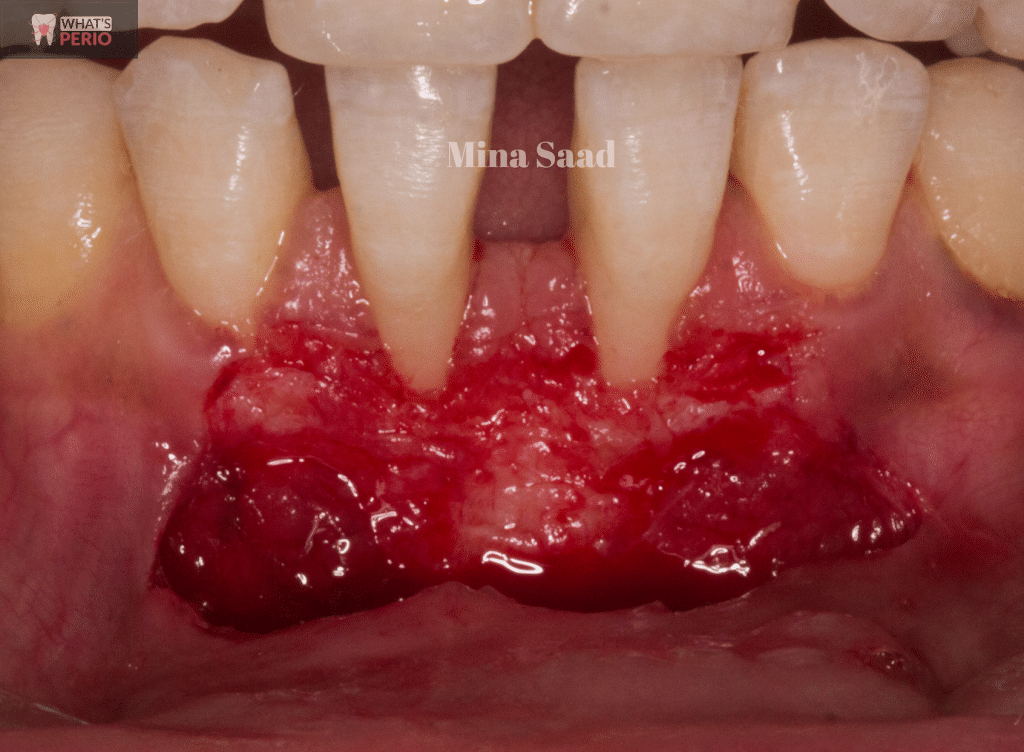
Vascular bed preparation to receive the free gingival graft. "recipient site"
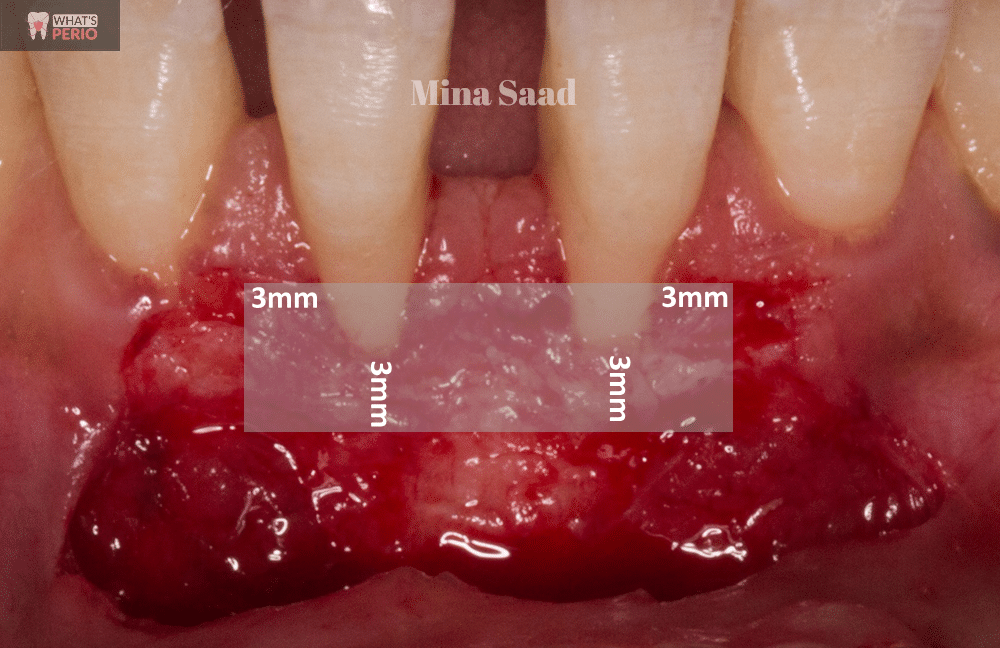
Graft must cover at least 3 mm of the vascular bed (mesial, distal & apical) to the exposed root surfaces..... So the vascular bed should be bigger than the graft size
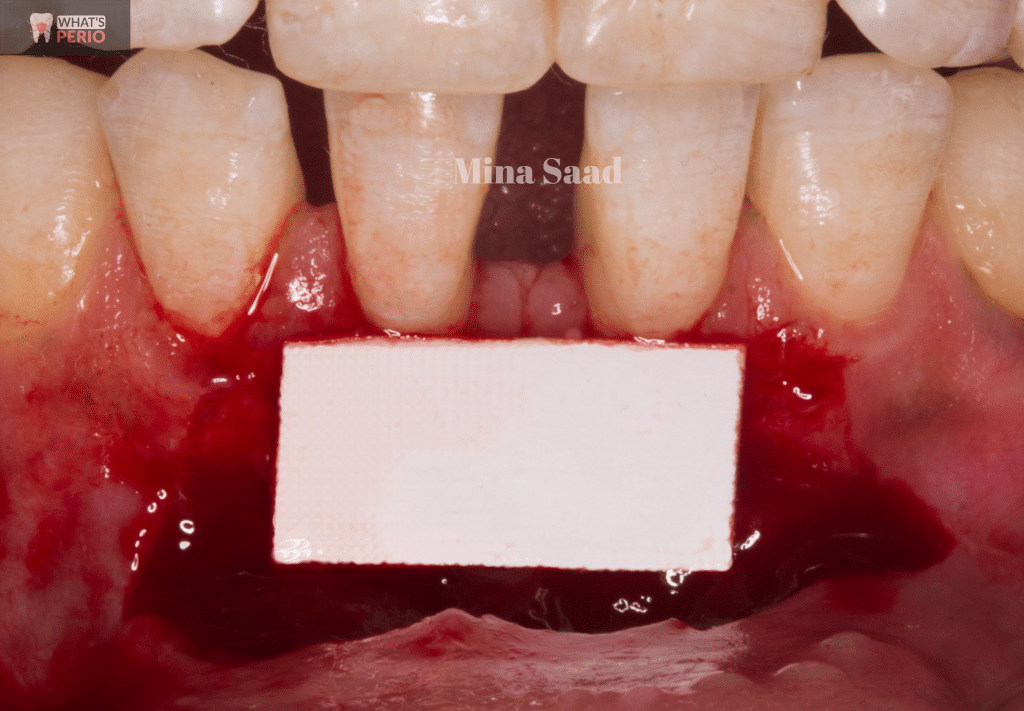
A template to measure the graft size.
The template placed over the recommended site.(donor site)
"Midway between median palatine raphe & distal to the free gingival margin of upper canine"

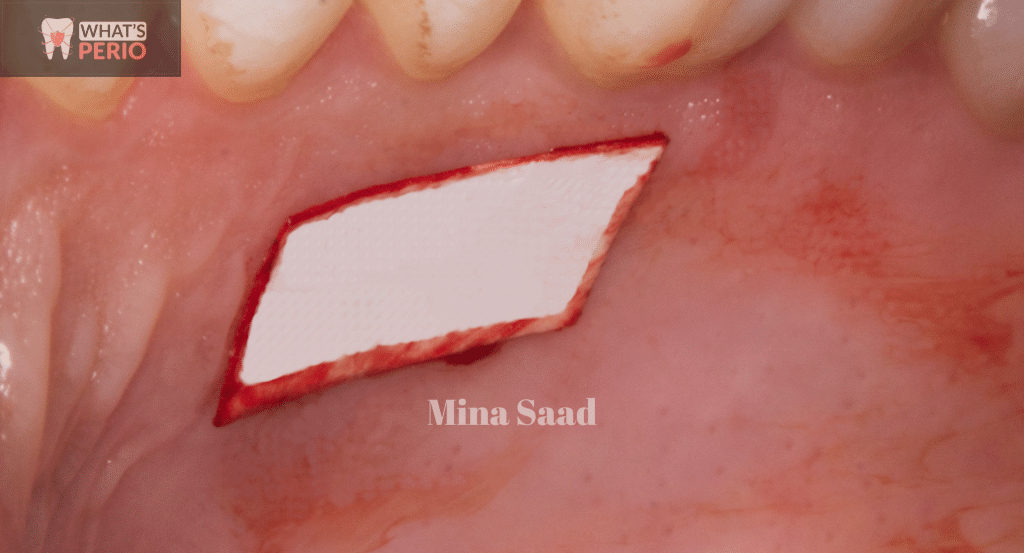
Incisions made for graft harvesting.
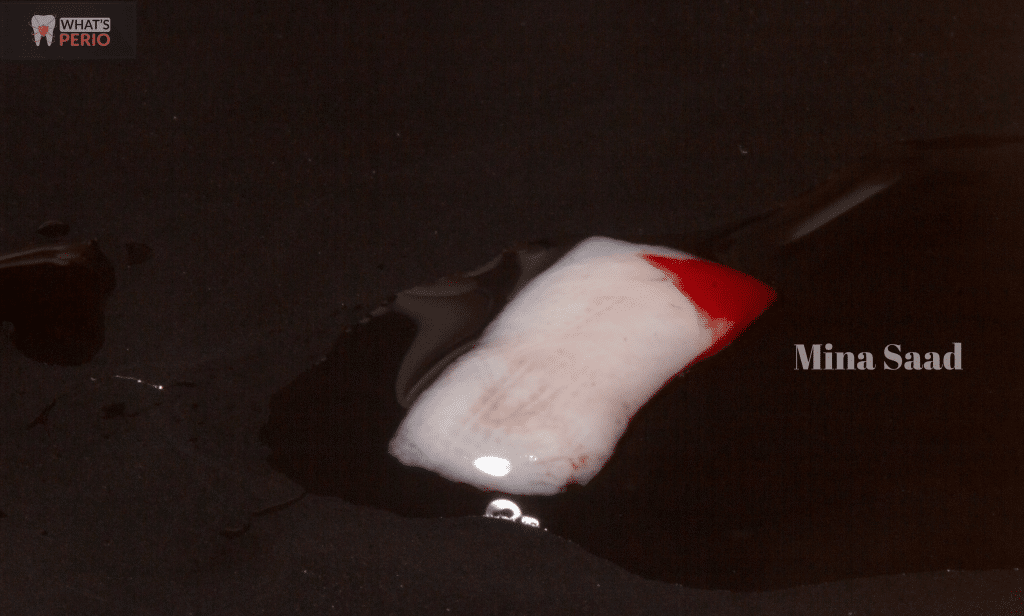
The graft after harvesting. "always keep it wet till delivering into the recipient site"
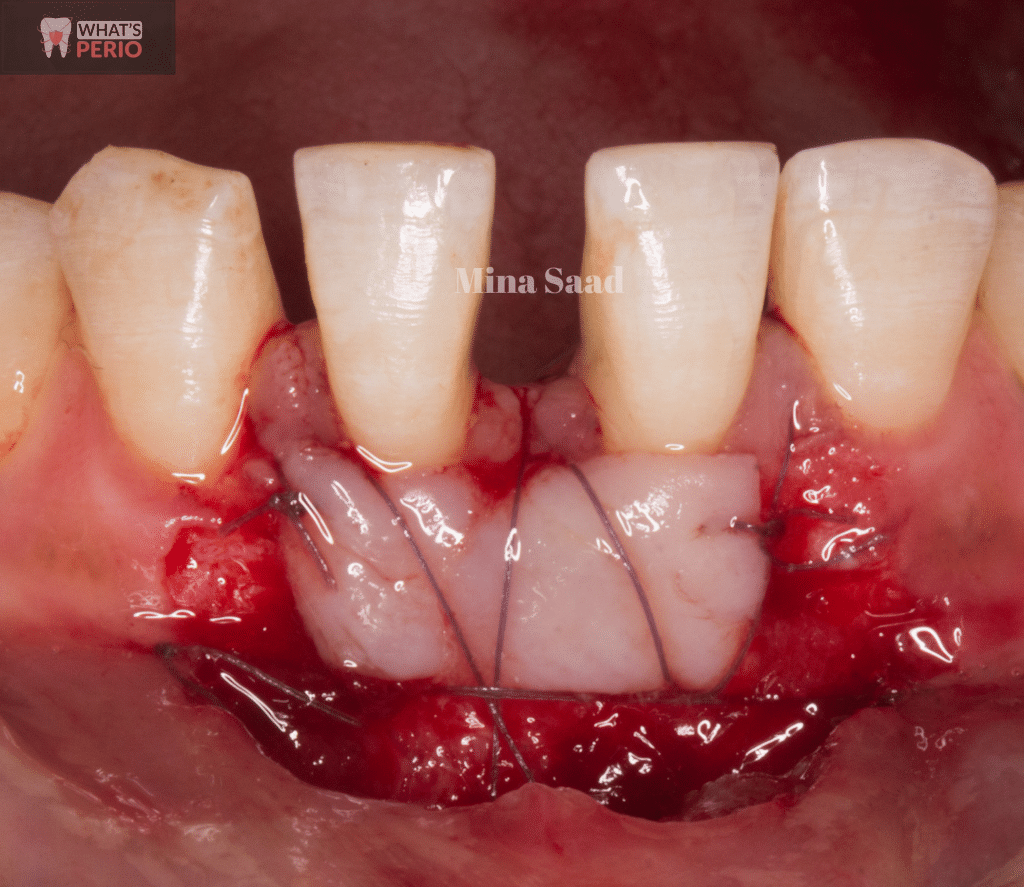
Securing the graft over the exposed roots & vascular bed.

Acrylic Stent prepared to cover the donor site.
"Note that the borders of the Stent are drawn on the cast to guide the technician during its fabrication"


"1st week follow up"
A whitish layer was formed on the external surface of the graft

The coronal graft margin fits snugly over the exposed roots by the criss cross sutures to avoid blood clot contamination.
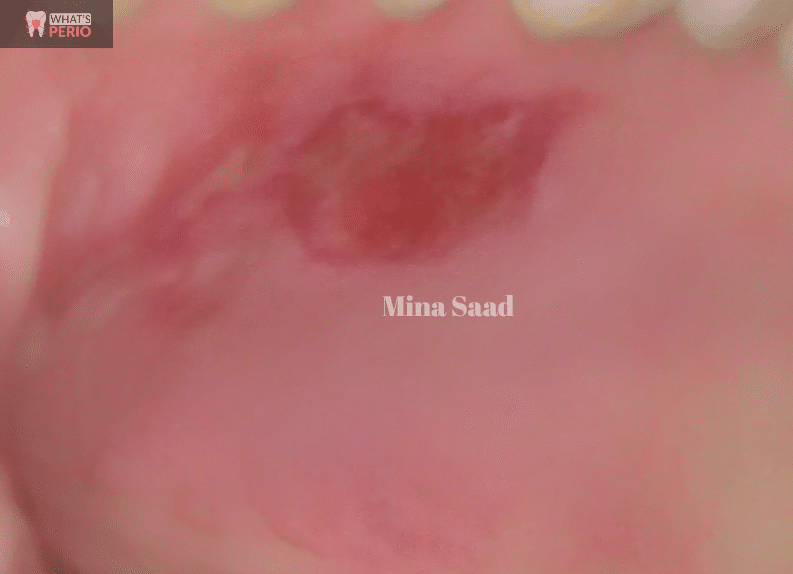
The donor site started epithelization.
"2nd week follow-up"
The graft started repithelization
Edit

The donor site continued to heal as it became more pale red in color and epithelization increased.
"3rd week follow up"
As the time passes, the graft takes on the color & surface features of the palatal mucosa from which it is harvested.
The donor site healing in the 3rd week

"1 month follow-up"

Complete healing of the donor site after 1 month

"2 months follow-up"

"3 months follow up"

Recession depth (RD) measurements began to decrease
RD for right central =2.5 mm.
RD for left central = 1.5 mm.


"4 months follow - up"

RD measurements decreased more in the 4th month
RD for right central = 1.5 mm.
RD for left central = 1 mm.

"5 months follow up".

RD measurements were the same as the 4th month.

Width of Keratinized gingiva (WKG) measurements increase after 5 months
Interdentally = 9.5 mm.
Right central = 5 mm.
Left central = 6 mm.
Edit

The gradual decrease in recession depth measurements were due to Creeping attachment occurred.
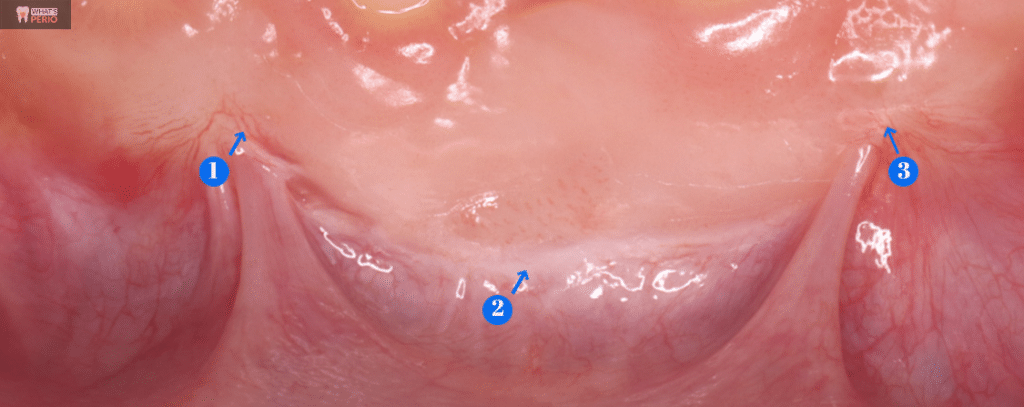
1 & 3 the arrows refer to blood vessels bridging between the gingiva & grafted tissue.
2... The arrow refers to the final location of the muco gingival junction (MGJ) below the grafted tissue.

Before & After 5 months.. and still the case is under follow up
Share on: