Static guided endodontics has emerged as a transformative technique in the management of pulp canal obliteration (PCO), a condition that poses significant challenges even for experienced clinicians. PCO, commonly resulting from dental trauma, aging, or restorative interventions, leads to progressive calcification of the root canal system, increasing the risk of missed canals, perforations, and extended treatment times during conventional endodontic procedures.
A recent randomized controlled clinical trial published in BMC Oral Health provides compelling in-vivo evidence that static guided endodontics (SGE) significantly enhances precision and safety in accessing obliterated canals compared with traditional freehand approaches. By minimizing procedural risks and optimizing canal negotiation, SGE offers endodontists a reliable method to improve both clinical outcomes and patient experience.
This article reviews the 2025 study by Li et al., highlighting the clinical implications of static guided endodontics in modern endodontic practice and its potential to redefine management strategies for teeth affected by PCO.
Static Guided Endodontics In Managing Pulp Canal Obliteration
What is Pulp Canal Obliteration?
Pulp Canal Obliteration (PCO) is a condition where the pulp chamber and root canals, the hollow spaces inside a tooth that contain nerves and blood vessels, become filled with hard tissue. On an X-ray, the canal appears to have vanished or become extremely narrow. This can be triggered by:
-
Dental trauma
-
Extensive cavities and restorations
-
Certain dental procedures, like vital pulp therapy
-
Natural, age-related changes
The problem arises when a tooth with PCO becomes infected or necrotic (dies). To perform a life-saving root canal, an endodontist must navigate these hidden, calcified canals. Traditionally, this is done freehand using a dental operating microscope (DOM), CBCT scans for a 3D view, and specialized ultrasonic instruments. Despite these advanced tools, the process remains exceptionally challenging, relying heavily on the clinician’s skill and feel, and often requiring the removal of more healthy tooth structure than desired to find the elusive canal.
Uncovering The Hidden Third Set of Teeth By Dr Takahashi
What is Static Guided Endodontics?
Static guided endodontics (SGE) is a minimally invasive, technology-driven approach that brings the precision of computer-aided surgery to root canal treatment. Think of it as a GPS for a dentist’s drill.
The process involves:
-
3D Imaging: A Cone-Beam CT (CBCT) scan is taken to create a detailed 3D model of the tooth and its hidden, calcified canal.
-
Digital Planning: Specialized software is used to merge CBCT data with a digital impression (intraoral scan) of the patient’s dentition, allowing precise virtual planning of the most conservative and accurate access path to the canal. Commonly used platforms for static guided endodontics include:
-
coDiagnostiX® (Dental Wings): widely used for designing static guides and planning access cavities.
-
Planmeca Romexis®: integrates CBCT and intraoral scans for comprehensive endodontic treatment planning.
-
3Shape Implant Studio®: Though primarily for implant planning, it is increasingly applied for guided endodontic access design.
-
Exocad® DentalCAD: supports merging CBCT with scans and designing precise guide sleeves for endodontic procedures.
These software tools allow the endodontist to simulate the canal trajectory, minimize dentin removal, and ensure safe, predictable treatment outcomes before any clinical intervention.
-
3D-Printed Guide: Based on this digital plan, a custom, tooth-supported surgical guide is 3D-printed. This guide fits snugly over the tooth and contains metal sleeves that precisely direct the drill bur along the pre-determined path.
While SGE has been used successfully in case reports for nearly a decade, its superiority lacked validation from high-quality, in-vivo (in living patients) randomized controlled trials, until now.
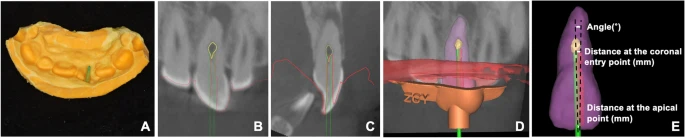
Virtual planning of the access cavity. (A-C) CBCT image displays a severely calcified root canal (indicated in yellow) of the upper central incisor (highlighted in purple). The virtual template (outlined in orange) and virtual bur (represented by a green cylinder) are positioned within the conservative endodontic access cavity range. (D-F) The virtual template (depicted in orange) is utilized in software to plan the identification of the calcified root canal (shown in yellow) in the upper central incisor
The Groundbreaking Study: A Closer Look at the Methods
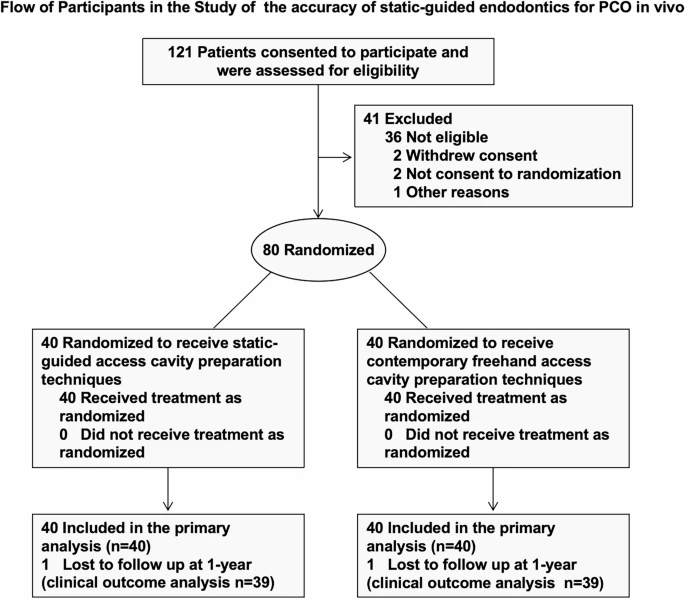
The study, led by Jiayang Li and colleagues, was designed to fill this critical evidence gap. It involved 80 patients with PCO who needed root canal treatment. They were randomly assigned to one of two groups:
-
The Static-Guided Group: Underwent access cavity preparation using a 3D-printed endodontic guide.
-
The Freehand Group: Underwent traditional access cavity preparation using a dental operating microscope, considered the contemporary standard of care.
The research team introduced an innovative method to measure accuracy. Instead of relying on post-operative CBCT scans (which expose patients to additional radiation), they used precise indirect impression scans of the prepared access cavities. These scans were digitally compared to the original virtual plan to measure deviations down to a fraction of a millimeter.
The primary goal was to measure accuracy, while secondary goals assessed patient pain during treatment and clinical success rates after one year.
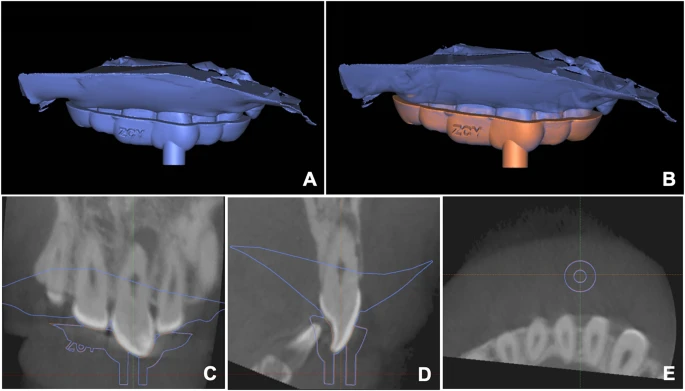
The assessment of guide template accuracy prior to surgery. (A) Intraoral scanning (depicted in blue) after the placement of the template guide. (B) The intraoral scan was registered to the virtual plan based on the teeth. The template was superimposed on the virtual template (depicted in orange), ensuring precise alignment with the surgical plan and enabling complete simulation transfer. (C-E) A virtual template (orange outline) and intraoral scanning after the placement of the template guide (blue outline) were superimposed in software
The Results: A Clear Winner in Precision
The findings were striking and statistically significant.
Unmatched Accuracy of Guided Endodontics
The static-guided group demonstrated exceptional precision:
-
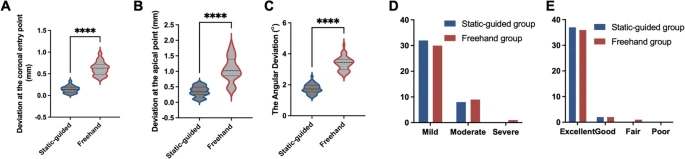
Coronal Entry Point Deviation: 0.14 ± 0.08 mm
-
Apical Point Deviation: 0.35 ± 0.16 mm
-
Angular Deviation: 1.75 ± 0.30°
In contrast, the freehand group showed much larger deviations:
-
Coronal Entry Point Deviation: 0.62 ± 0.15 mm
-
Apical Point Deviation: 1.06 ± 0.39 mm
-
Angular Deviation: 3.38 ± 0.44°
The statistical analysis confirmed that the static guided approach was significantly more accurate at every measured point (P < 0.0001). This level of precision in a clinical setting is unprecedented and highlights the potential of SGE to eliminate common mishaps like perforations or missed canals.
Enamel Regeneration Research : The Future Of Smiles
Patient Experience and Long-Term Outcomes
Interestingly, the study found no significant difference between the two groups in terms of pain during treatment or the clinical success rate at the one-year follow-up.
-
Pain Levels: Patients in both groups reported similar levels of discomfort, with the majority experiencing only mild pain. This suggests that while SGE is more precise, it does not add to the patient’s discomfort during the procedure.
-
Success Rates: An impressive 98.7% of all participants had favorable outcomes (rated “excellent” or “good”) after one year. The single less favorable outcome was observed in the freehand group; however, the difference between groups was not statistically significant.
The researchers hypothesize that while the one-year outcomes are similar, the long-term benefits of SGE, such as better preservation of tooth structure leading to stronger teeth, may become more apparent with longer follow-up periods.
Clinical images during treatment. (A) It is noted that standard rubber dam isolation is consistently implemented for all cases. (B) A template accompanied by a metal sleeve #1 is utilized to ensure accurate and reproducible fitting on the teeth. (C) The teeth are equipped with a template accompanied by metal sleeve #1 to facilitate the removal of enamel and exposure of dentin, utilizing a round diamond bur. (D) The resulting image showcases the endodontic access cavity after the initial bur has been employed. (E) The template is replaced by metal sleeve #2. (F) A low-diameter bur is utilized in a pecking motion to drill through the metal sleeve #2, thereby achieving the desired path length. (G) View of the endodontic access cavity after root canal location. (H) The guide direction is consistent with the root canal direction
Why This Study is a Game-Changer for Dental Care
This research is more than just a confirmation of a technique’s accuracy; it represents a paradigm shift in how complex endodontic cases can be managed.
-
Validates In-Vivo Efficacy: This is the first robust clinical trial to prove that the accuracy demonstrated in lab studies translates directly to successful patient treatment.
-
Introduces a Novel Measurement Technique: The use of indirect impression scans provides a safe, reliable, and radiation-free method for measuring procedural accuracy in future clinical studies.
-
Enhances Predictability: For clinicians, SGE reduces the guesswork and stress associated with treating PCO. It provides a predictable, reproducible pathway to the canal, which is especially valuable for less experienced dentists or exceptionally complex cases.
-
Paves the Way for Minimally Invasive Dentistry: By allowing for a more precise and conservative access cavity, SGE helps preserve the tooth’s natural integrity. A stronger tooth is less prone to fracture and has a better long-term prognosis, a factor future studies are poised to quantify.
🎼 The Way Beethoven Used His Teeth to Hear His Music
The Future of Guided Endodontics
While this study firmly establishes SGE as a superior technique for accuracy, the authors note there is always room for refinement. Future research directions include:
-
Long-Term Follow-Ups: Tracking patients over 5 or 10 years to see if the precision of SGE translates into higher long-term survival rates.
-
Tooth Structure Analysis: Quantifying exactly how much more tooth structure is preserved with SGE compared to the freehand method.
-
Technical Refinements: Exploring improvements like magnetically-attached guides to eliminate even minor potential errors during guide handling.
(A) Following access cavity preparation, indirect impression scanning of the access cavities was executed. (B-D) Indirect impression scanning was aligned with the pre-operative model to gauge the qualitative precision. CBCT images display a severely calcified root canal (yellow outline), the virtual access cavity (green outline), and the executed access cavity (red outline). (E) A representative scheme of the measurements in linear deviation and angular deviation
Conclusion: A New Standard of Care for Complex Root Canals
The 2025 clinical trial by Li et al. provides compelling evidence that static-guided endodontics is not just an alternative, but a profoundly superior approach for locating calcified canals in teeth with pulp canal obliteration. With its demonstrated deviations of under half a millimeter, SGE offers a level of precision that the freehand method simply cannot match.
For patients facing the prospect of a root canal on a calcified tooth, this technology means a safer, more predictable, and potentially less invasive procedure. For the dental community, it marks the arrival of a powerful new tool that elevates the standard of care, turning one of dentistry’s most challenging procedures into a planned and precise intervention.
As this technology becomes more widespread, it promises to improve outcomes, reduce anxiety, and help patients keep their natural teeth healthy and functional for a lifetime.
The Use of Laser in Precipitating Nano-MTA on Dentine Root Surface
Source:
Accuracy of static-guided endodontics for access cavity preparation with pulp canal obliteration: a randomized controlled clinical trial
Jiayang Li, Yufeng Hu, Zhifei Ma, Hui Liu, Liqun Cao & Xiaoling Wei BMC Oral Health volume 25, Article number: 933 (2025)
Broken Endodontic Files: Causes, Implications, and Retrieval Strategies
In-Situ Direct 3D Bone Grafting: The Future of Bone Repair
Biomimetic Pins and Screws: Advancements in Dental Surgery
Treating TMJ Arthritis with Collagen Injection
How Sustainable Dentistry is Tackling Climate Change
Share on: